5-Fluorouracil as an Adjunct in Glaucoma
Filtration Surgery in Younger Age Group
Norin Iftikhar Bano, Tariq Mehmood Qureshi, Muhammad Tariq Khan, Harris Muzammil Ansari
Pak J Ophthalmol 2011, Vol. 27 No. 1
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . See end of article for Purpose: To evaluate efficacy and complication of 5-Flourouracil (5-FU) as an authors affiliations adjunct in trabeculectomy in young age group.
Material and Methods: 86 eyes of 62 patients were included in the study. There
…..………………………..
were 48 male patients (55.81%) and 38 female patients (44.18%). Age of Correspondence to: patients were two year to fifteen year. Duration of study was four years with Norin Iftikhar Bano average follow up of two years.
LRBT Free Eye & Cancer Study was conducted at LRBT Eye Hospital Lahore. Trabeculectomy was
Hospital
436-A/I, Township performed with conventional method. First subconjuctival injection of 5-FU (50mg/0.2ml) was given at the end of the procedure, second at the end of 1st
Lahore
week and the third at the end of 2nd week. Additional 1-2 injections of 5-FU were
given in more resistant cases. Results: Target IOP was achieved in 83 (96.51%) of patients, 2 (2.32%) patients were given additional medication to achieve target IOP and 1 (1.16%) did not achieve target IOP. Visual acuity remained stable in 69 (80.23%) patients, improved in 13 (15.12%) patients, while it deteriorated in 4 (4.65%) patients due to late complications. Cup-to-disc ratio reversal was seen in 30% patients up to 14 years of age
Choroidal detachment occurred in 8 (9.30%) patients and was successfully
treated with cycloplegics and pressure patching. Choroidal drainage was done in Received for publication only one patient. Thin bleb was seen in 4 (4.65%) patients. Blebitis occurred in 1 June’ 2010 (1.16%) patient that led to endophthalmitis. 2 (2.32%) patients had retinal …..……………………….. detachment. Redo-trabeculectomy was done in 3 (3.48%) cases.
The surgical trabeculectomy has been prototype cally mediates its antiproliferative effect by
glaucoma filtering procedure over the last three antagonizing pyrimidine metabolism; hence is decades2. Primary trabeculectomy is still a preferred classified as an antimetabolite. 5-Fluorouracil is active
surgical approach all over the world for cases in which on the synthesis phase of cell cycle. Fibroblastic a larger reduction in IOP is the aim of treatment, proliferation is inhibited while fibroblastic attachment
especially when high IOP persists, despite maximum and migration are unaffected6. tolerable anti -glaucoma medication3,7. We conducted this study to overview the efficacy At times, certain co-existing risk factors (e.g. and complications of 5-Fluorouracil as an adjunct in
young age, uveitis, trauma) can result in failure in glaucoma surgery in younger age groups. even the primary trabeculectomy4. Such cases
12
MATERIAL AND METHODS
This was a hospital based study conducted at the LRBT Free Eye and Cancer Hospital Lahore from January 2005 to June 2010. Patients with a minimum of two years follow up were included in this study. Eighty six eyes of 62 patients were included in this study.
Patients with Congenital glaucoma, glaucoma due to use of steroids, (responders), post traumatic glaucoma and those with previously failed trabecu-lectomy were included in the study.
Patients with neovascular glaucoma, active iritis or scarred superior fornix were excluded from the study.
Preoperative evaluation; For those upto six years of age 90% of examination was carried under sedation with Chloral hydrate (500mg/5ml). During examina-tion IOP was measured with Perkins applana-tion tonometer, corneal diameter with calipers and detailed fundus examination especially cup-disc ratio was done with indirect or direct ophthalmoscope. Older cooperative children were examined routinely on slit lamp.
Preoperatively the intraocular pressure was controlled with topical beta blockers and topical carbonic anhydrase inhibitor, however in some cases a third topical anti-glaucoma drug like alpha agonist above the age of two year was also used. In some cases preoperative intravenous Mannitol was used for rapid control of IOP.
Operative procedure: Trabeculectomy was performed in each eye according to a modification of the technique developed by Watson and Cairns. After making a fornix based conjunctival flap, partial thickness rectangular scleral flap (4mm wide by 3mm long.) was made, block of deep sclera (2mm wide by 1.5mm long) was excised and peripheral iridectomy performed. The superficial scleral flap was approximated; Conjunctiva and tenon were sutured separately. Subconjunctival injection of 5-FU (50mg/0.2ml) was given in a separate plane directed away from the fistula. Eye washed thoroughly to remove any released 5-FU to prevent epithelial toxicity which was reported to be very high with 5-FU.
Second injection of 5-FU was given after first week and third after second week. Additional 1-2 injections of 5-FU were given if found necessary.
Postoperative care: On the first postoperative day, intraocular pressure was recorded with computed air-puff tonometer. In cases of shallow anterior chamber a cycloplegic was used and if the anterior chamber was not formed properly, a pressure bandage with antibiotic eye ointment was used for another twenty four hours.
Postoperatively topical antibiotic and steroid eye drops were used every two to four hours in waking hours and antibiotic eye ointment at bed time if necessary. The treatment was tapered off according to condition of the eye on follow up visits. Postoperative follow-up was at week 1, 2, 6 and at the 3rd month and then 6 monthly. At each visit visual acuity was recorded and slit lamp biomicroscopic examination was carried out to evaluate the condition of conjunctiva, cornea, anterior chamber, vitreous, macula and optic disc. Applanation tonometry was done and corneal diameter was recorded. Special emphasis was given at the condition of bleb i.e. which type of bleb is established and the vascularisation of the bleb, and to decide how many postoperative subconjunctival injections of 5-FU should be given.
5-FU used in concentration of 50mg/0.2ml with 27 gauge needle on insulin syringe, given 10 to 12 mm away from the bleb. Total dose of 5-FU ranged from 15 to 25mg per patient. In 90% of the cases only three injections were required.
RESULTS
Eighty six eyes of 62 patients were included in the study. There were 48 male patients (55.81%) and 38 female patients (44.18%) (Table 1). Duration of study was four years with average follow up of two years.
Table 1:
| Age (Years) | Number of Eyes | Total eyes | |
|---|---|---|---|
| Male | Female | ||
| 2-5 | 18 | 15 | 33 |
| 6-10 | 17 | 10 | 27 |
| 11-15 | 13 | 13 | 26 |
| Total | 48 | 38 | 86 |
Target IOP was achieved in 83 (97%) of patients, additional 2 (2%) patients also achieved target IOP with AGT and 1 (1%) did not achieve target IOP (Fig. 1). Vision remained stable in 69 (80%) patients, in 13
13
| (15%) | patients | it | improved | while | in | 4 | (5%) | it | occurred in 8 (9.30%) patients, most of these patients |
| deteriorated (Fig. 2). | had microspheric lens. Choroidal drainage was done | ||||||||
| in two cases, other six responded well with pressure | |||||||||
| patching, cycloplegics and steroids. Thin bleb was | |||||||||
seen in 4 (4.65%) patients. Blebitis occurred in 1 (1.16%) patient that led to endophthalmitis. Retinal detachment occurred in 2 (2.32%) patients. Redo trabeculectomy was done in 3 (3.48%) cases because stitches were not released in time due to poor follow up (Fig. 3).
DISCUSSION
The main cause of failure of filtering surgery is scarring of the filtering bleb. Antimetabolites like 5-FU and MMC originally found to inhibit scarring through their inhibitory effect on fibroblasts, are efficacious after filtering surgery in preventing bleb fibrosis in
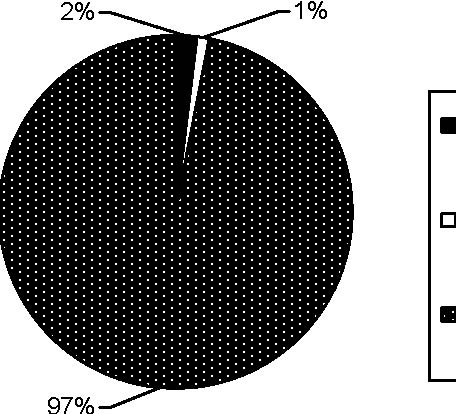
Achieved
Achieved with AGT
Not Achieved
Fig. 1: Target IOP
eyes with poor surgical prognosis10.
The prognosis of glaucoma surgery is poor in
![]() 100
100
50
0
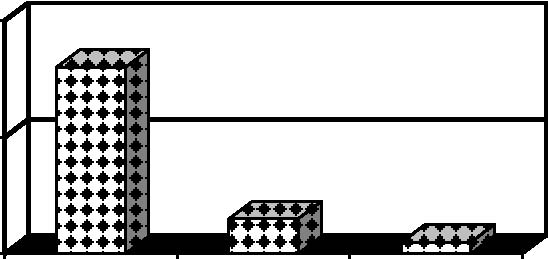
Stable Improved Deteriorated
Fig. 2: Post Trabeculectomy Visual Acuity complicated cases such as previous failed trabeculectomy, inflammatory glaucoma, angle recession glaucoma, combined procedure, younger age group, history of topical anti glaucoma medication for more than three years, previous history of conjunctival surgery and individuals with dark skin.
This effect is caused by inhibition of fibroblast proliferation or inhibition of cell migration and extracellular matrix production. As a result of its
prolonged cytological toxicity, MMC is associated with development of potentially severe side-effects and complications as compared to 5-FU. It may lead to development of thin walled avascular bleb which may
results in over filtration. Late onset focal bleb leaks are three times more frequent with Mitomycin C than with 5-FU13. Such blebs are strongly associated with endophthalmitis. The posterior choroid becomes
thickened in acute hypotony followed by choroidal detachment. Sclerits is also reported in some patients13. Although MMC is an effective antifibrotic adjunct with glaucoma surgery but there is a growing concern with hypotony, leaky ischemic blebs, and potentially increased risk of endophthalmitis. This has led us to re-evaluation of the use of 5-FU.
30
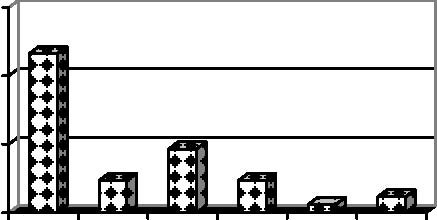
Percentage of Patients
20
10
0
Fig. 3: Complications
In our study, a complete surgical success was considered to be an intraocular pressure of less than 21 mm Hg without any anti-glaucoma medication after
Cup-to-disc ratio reversal was seen in 30% of the
patients. Shallow anterior chamber was seen in 20 trabeculectomy with 5-FU. We also studied the safetyeyes, treated with cycloplegics and pressure patching. of use of 5-FU.Epithelial toxicity was found in 4 patients that was
reduced with the application of ointment for three Pressure rose in those cases in which we were days after injection of 5-FU. Choroidal detachment unable to give inj. 5-FU due to choroidal detachment
14
or poor follow up of the patient. We had to redo in these cases in spite of 3- 5 injections of 5-FU.
Chronic hypotony was seen in only one case in which the cause of glaucoma was angle recession, Intravitreal C3F8 was injected, that brought the IOP to 12mmHg but vision did not improve due to maculopathy.
Thin cystic bleb was seen in 4 cases that were managed with postoperative lubricants. Blebitis was seen in one case, that child had iridocorneal endothelial syndrome. The present study has clearly demonstrated that 5-FU improves the surgical prognosis for patients at low to moderate risk as well as high risk for failure and indicates that 5-FU facilitates filtering bleb formation as well as with less complications.
There is a significant benefit of 5-FU, in terms of bleb survival and clinical success as determined by IOP. According to national survey of antimetabolite 93% of consultants are using 5-FU rather than MMC in United Kingdom14. There are some differences between success rates of different studies yet our study results are comparable to that demonstrated in some of the previous studies.
Among previous studies, the pilot study of Heuer and colleagues with postoperative subconjunctival injections daily for up to two weeks showed the success rate in previous failed trabeculectomy was found 81%16. Although the results of these studies are comparable with our study yet the number of postoperative injections was quite higher compared to our study17. Leibmann showed 77.8% 5 years success rate18.
Our complications with the use of 5-FU were less as compared with other studies. The cause seems to be less number of subconjunctival injections.
CONCLUSION
The use of 5-FU as an adjunctive has a significant efficacy and low complication rate in glaucoma filtration surgery.
Author’s affiliation
Dr. Norin Iftikhar Bano LRBT Free Eye & Cancer Hospital 436-A/I, Township Lahore Dr. Tariq Mehmood Qureshi LRBT Free Eye & Cancer Hospital 436-A/I, Township Lahore
Dr. Muhammad Tariq Khan LRBT Free Eye & Cancer Hospital 436-A/I, Township Lahore
Dr. Harris Muzammil Ansari LRBT Free Eye & Cancer Hospital 436-A/I, Township Lahore Dr. Khalid Mehmood LRBT Free Eye & Cancer Hospital 436-A/I, Township Lahore
REFERENCE
- Kanski JJ. Clinical ophthalmology. A systematic approach. 5th ed. Oxford: Butterworth Heinemann. 2003: 259.
- Lama PJ, Fecther RD. Antifibrotic and wound healing in glaucoma surgery. Surv Ophthalmol. 2003; 48: 314-46.
- Jalal T, Mohammad S. Three years retrospective study of patients undergone trabeculectomy in Lady Reading Hospital Peshawar. J Postgrad Med Inst. 2004; 18: 487-94.
- AGIS Investigators. The Advanced Glaucoma Intervention Study (AGIS): 11. Risk factors for failure of trabeculectomy and argon laser trabeculoplasty. Am J Ophthalmol. 2002; 134: 481
- 98.
- Fraser S. Trabeculectomy and antimetabolites. Br J Ophthalmol. 2004; 88: 855.
- Yorston D, Khaw PT. A randomized trial of the effect of intraoperative 5-FU on the outcome of trabeculectomy in east Africa. Br J Ophthalmol. 2001; 85: 1028-30.
- Iqbal Z, Khan N, Islam ZU. Glucoma, presentation and management at Khyber Teaching Hospital, Peshawar. J Postgrad Med Inst. 2002; 16: 211-4.
- The fluorouracil filtering study group. Fluorouracil filtering surgery study. One year follow up. Am J Ophthalmol. 1995;
- 108: 625-35.
- Ticho U, Ophir A. Late complications after glaucoma filtering surgery with adjunctive 5-fluorouracil. Am J Ophthalmol. 1993;
- 115: 506-10.
- Jamper HD, Jabs DA, Quigley HA. Trabeculectomy with 5-Fluorouracil for adult inflammatory glaucoma. Am J Ophthalmol. 1990; 109: 168-73.
- Khaw PT, Doyale JW, Sherwood MB. Prolonged localized tissue effects from 5 minutes exposures to fluorouracil and mitomycin-c. Arch Ophthalmol. 1993; 111: 263-7.
- Khaw PT, Sherwood B, Mackay LD. 5 minute treatment with fluorouracil, floxuridine and mitomycin-c have long term effect on human tenon’s capsule fibroblasts. Arch Ophthalmol. 1992;
- 110: 1150-4.
- Lachkar Y, Leyland M, Bloom P, et al. Trabeculectomy with intraoperative sponge 5-fluorouracil in Afro-Caribbeans. Br J Ophthalmol. 1997; 81: 555-8.
- Lama PJ, Fechtner RD. Antifibrotics and wound healing in glaucoma surgery. Surv Ophthalmol. 2003; 48: 314-46.
15
- Siriwardena D, Edmunds B,Wormald RPL, et al. National mitomycin-c. A comparative study with fluorouracil. Arch survey of antimetabolite use in glaucoma surgery in Unitted Ophthalmol. 1991; 109: 1693-42. Kingdom. Br J Ophthalmol. 2004; 88: 873-76. 21. Skuta GL, Beeson CC. Intraoperative mitomycin-c vs.
- Lachkar Y, Leyland M, Bloom P, et al. Trabeculectomy with Postoperative 5-Fluorouracil in high risk glaucoma filtering intraoperative sponge 5-fluorouracil in Afro-Caribbeans. Br J surgery. Ophthalmology. 1992; 99: 438. Ophthalmol. 1997; 81: 555-8. 22. Zacharia PT, Depperman SR. Ocular hypotony after
- Heuer DK, Parrish RK, Gressel MG. 5 Fluorouracil and trabeculectomy with mitomycin-c. ARVObstracts Ophthalmol glaucoma filtering surgery: Intermediate follow up of a pilot Vis Sci Philadelphia, JS Lippincott. 1993: 816. study. Ophthalmology. 1986; 93: 1537-46. 23. Kitazawa Y, Kawase K, Matsushita H. Trabeculectomy with
- Goldenfeld M, Krupin T, Ruderman JM. 5 Fluorouracil in mitomycin-c. A comparative study with fluorouracil. Arch initial trabeculectomy: A prospective, randomized, multicenter Ophthalmol, 1991. 109: 1693-8. study. Ophthalmology. 1994; 101: 1024-29. 24. Suner IJ, Greenfild DS, Miller MP, et al. Palmberg PF, 1997.
- Greenfield DS, Liebmann JM, Jee J, et al. Late onset bleb leaks Ophthalmology. 1997; 104: 207-14. after glaucoma filtering surgery. Arch Ophthalmol. 1998; 116: 25. Ehrlich R, Snir M, Lusky M, et al. Augmented trabeculectomy 443-7. in paediatric glaucoma. Br J Ophthalmol. 2005; 89: 165–8.
Kitazawa Y, Kawase K, Matsushita H. Trabeculectomy with
16