Ptosis with poor levator function has always been challenging for
an ophthalmologist or an oculoplastic surgeon. There are many options for its
correction1. Usually, frontalis brow suspension is used for
correction of ptosis with poor levator function2. Although other
procedures like levator resection3 alone or combined with tarsectomy4
have also been successfully tried in this regard, however most ophthalmologist
agree on the superiority of frontalis sling for correction of ptosis with poor
levator function.
Unilateral ptosis with poor levator function usually creates a
dilemma for the surgeon. For long it has been advocated that the fellow normal
eye must also undergo brow suspension to avoid any asymmetry. The decision of
operating a normal eye is not easily accepted by the patient. In this study we
performed unilateral frontalis suspension in patients having ptosis with poor
levator function to assess the asymmetry in primary position.
MATERIAL AND METHODS
Thirty eyes of 30 patients were included in the study. The study
was done at Oculoplasty clinic, Al-Ibrahim Eye Hospital, Isra Postgraduate
Institute of Ophthalmology. Patients were included from January 2006 to
December 2008. Patients were followed up for two years at regular intervals to
look for subsequent complications and delayed failure. All the patients
reporting at the institute for correction of unilateral congenital ptosis with
poor levator function (i.e. less than 5 mm)5 were included. Among
these, some patients were excluded on the basis of having poor bell’s
phenomenon, Marcus Gunn jaw winking, 3rd nerve misdirection, squint,
impaired corneal sensitivity and neoplastic lesions.
Patients with simple congenital ptosis were diagnosed clinically
on the basis of history, old photographs and clinical signs i.e. ptosis,
absence of lid crease and defective levator function.
Pre-operative assessment included a proper history including
personal biodata, relevant information and an informed consent. A detailed
ocular and general examination was performed with special emphasis on the lid
measurements such as vertical fissure height (VFH), marginal reflex distance in
primary gaze (MRD), levator function (LF) and marginal limbal distance (MLD).
Associated features such as Bell’s phenomena, jaw winking, corneal sensitivity
status and evidence of any pre-existing inflammatory, infectious or neoplastic
lesion of the eyelids was noted. Pre operative photographs were taken. All the
information was recorded on a proforma.
Patients in whom procedure was done in general anesthesia, a
detailed physical examination was done and relevant investigations such as
complete blood count, random blood sugar and x-ray chest were done in
consultation with an anesthetist.
General anesthesia was used in children under 15 years. In adults
frontal block along with local infiltration along the track of the sling was
sufficient. Additional sedation or analgesics were not required in any case.
Sling was planned in a fox pentagon1 design. Skin was marked at five
points with gentian violet dye. Two marks were made along the lid margin, 2-3
mm superiorly near the medial and lateral extremes of the upper lid. Two brow
marks were made in the upper margin of the brow, the lateral one just lateral
to the lateral lid margin mark and the medial one just medial to the medial one
on the lid margin. The final mark was made 10 mm superior to the brow line over
the frontalis muscle in between the two brow marks. All marks were incised with
11 no. blade. 2/0 polypropylene (Prolene) suture was used as sling material.
Wright’s spatula needle was introduced through the incisions to drag the suture
along until the two ends meet at the final incision over the frontalis muscle.
Knot was tied by making sure that the lid margin stays at the level of superior
limbus. 5-6 knots were tied to decrease the chances of knot unwinding. The knot
was then buried deep under the frontalis muscle, by making a facial pocket, to
avoid knot exposure. The upper three incisions were closed with 6/0
polypropylene suture. The lower two incisions near the lid margin were left
unstitched as the close approximation of their lips by the sling rendered it
unnecessary. The sling was not anchored separately to the tarsal plate. A frost
suture was applied near the lower lid margin to close the lids and support the
sling. Eye was closed with sterile eye pad with antibiotic eye ointment.
On the first post-operative day, frost suture was removed. Photographs
were taken to record the outcome which was usually masked by some degree of lid
edema. Complications were looked for, especially lagophthalmos which was
relatively common but innocuous. Patients were discharged on oral NSAID’s,
topical lubricants and antibiotic drops for use on hourly or two hourly bases
depending on the amount of lagophthalmos. Topical antibiotic ointment was
prescribed for use at bedtime regularly.
Patients were followed on 1st post-operative week on which the
skin sutures on the upper three incisions were removed. After that they were
called on the 3rd week, then monthly for six months and then three
monthly for next one and a half years. On each visit complete examination was
performed to record the MRD, amount of lid lag, any signs of exposure keratitis
and delayed sling failure. Photographs were taken and examination recorded on
the proforma.
RESULTS
Thirty eyes of 30 patients were included in this study. All
patients had unilateral ptosis. Age of the patients ranged from 2 years to 41
years (average-18.73 years). 19 (63.33%) patients were male while 11 (36.66%)
were female. Levator function ranged from 0-4 mm (average 2.7 mm) 24 (80%) eyes
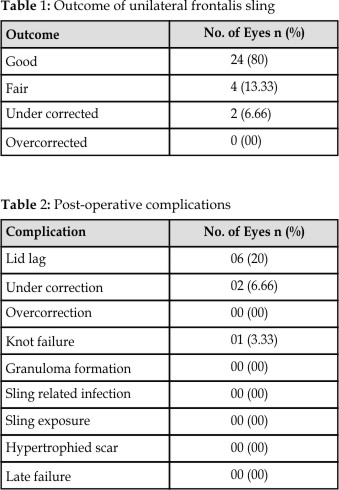
had good outcome (within 1 mm of normal), 4 (13.33%) had fair outcome (within 2
mm of normal) and 2 (6.66%) had under correction (table 1) but as the patients
were satisfied cosmetically, no second procedure was attempted. 6 (20%) eyes
had lagophthalmos, which subsided with time without any further sequel.
Exposure keratitis was not noted in any patient as the lagophthalmos was not
serious or prolonged. Frequent post-operative lubrication was also very
important in avoiding exposure keratitis. It was usual for lagophthalmos to
improve after one week as the lid edema would resolve significantly by then,
but even then lubrication with ointment at bedtime was continued. 1 (3.33%) eye
had knot failure (table 2), which showed up on the 1stpost-operative
week and was corrected by revising the sling procedure. All patients were
followed up for 2 years and no significant delayed failure or sling material
related complication such as extrusion, infection or granuloma formation was
noted.
DISCUSSION
Unilateral ptosis with poor levator function has always been
challenging for an oculoplastic surgeon. Bilateral frontalis brow suspension
has long been advocated for attaining symmetrical result. However it’s not easy
to convince any patient to operate upon his normal eye. No surgical procedure
is free of complications. Frontalis suspension is definitely no exception.
Frontalis brow suspension in unilateral ptosis has not been frequently
advocated6,7 as it was thought to create gross asymmetry between the
both eyes. However, in our study we found that in most of the cases the results
are cosmetically acceptable.
The post-operative elevation with some amount of excess skin fold
was invariably acceptable for the patients. Also we noted a decrease in the
amount of this excess skin fold with time as the post-operative edema settled
down. Few other studies have also shown promising results with unilateral
slings; however most of them have studied Caucasian8 and Oriental9
eyes. Our study comprised of South Asian eyes which might reflect minor
differences in anatomical details.
Use of fascia lata has long been advocated as sling material in
frontalis suspension, as being superior in giving good results and fewer
complications. However, in some circumstances the availability or harvesting of
fascia lata is not possible or feasible, such as in extremes of age and cosmetic
concerns. This opens the door to the option of using artificial materials for
sling. Various materials have been successfully tried in this regard. These
include silicon tubes10, expanded polytetrafloroethylene (ePTFE),11-13
braided polyester14, nylon15, mersilene and polypropylene16
suture and strips of eTPFE and mersilene17 mash. All these studies
have shown their relevant merits and complications.

Fig.
1a. Five years old patient having OD severe
ptosis with poor levator function

Fig.
1b. Same patient on 2nd (3 weeks
post-operatively) follow up.
We have tried a very common and easily available suture i.e.
polypropylene 2/0 for sling in frontalis brow suspension. This suture is a
synthetic, monofilamantous, non-absorbable suture usually used in oculoplastic
procedures in sizes of 5/0 or 6/0. The size of 2/0 is usually used in general
surgical procedures. It gives good cosmetic results as it allows minimal
fibrosis along suture tract. This suture has not been tried commonly so far.
The reason for this was not evident from literature review. However we have
successfully used it with excellent results.
We found the success rate very promising in terms of the final
upper lid level or final MRD. In our study 93.33% (28 eyes) have satisfactory
results. Among these 80% had good result i.e. their final MRD was within 1mm of
normal and 13.33% had fair result i.e. MRD within 2 mm of normal. All these
patients were cosmetically satisfied. These results are comparable to KKL Chong
et al9 (83.3%) and Kersten RC et al8 (95%).This
comparison sufficiently advocates the efficacy of procedure in south Asian
eyes.
We experienced few complications in our patients. The commonest
was lagophthalmos. We experienced lagophthalmos in 6 (20% eyes), but it was not
severe enough to cause exposure keratitis in any patient. Lagophthalmos tends
to improve with time and frequent use of lubricant drops and ointments
especially during sleep is mandatory to avoid exposure keratopathy as do in our
study. Post-operative lagophthalmos is usually attributed to overcorrection as
by Lee V and Konrad H18 and Kersten RC8, however in our
study there were no cases of overcorrection, hence we found the cause to be
related to severity of ptosis and poor levator function. We found lagophthalmos
as more of a sequel rather than a complication when we operate on eyes with
poor levator function. The sling’s syncytium with the frontalis muscle affords
good lid closure with a little effort. However during sleep lubrication is
vital in early post-operative period. We did not notice any prolong lid lag in
any patients. It usually resolved significantly on 2nd follow up
i.e. at the end of the 1stpost-operative week.
We experienced under correction in 6.66% (2 eyes), but as the
patients were cosmetically satisfied, review surgery was not performed. However
one patient (3.33%) presented in early post operative period with recurrence of
ptosis due to knot failure. Sling had to be repeated in that patient to regain
the symmetry successfully.
Apart from those above mentioned, we did not experience any
complications. We followed up our patients for two years but did not experience
delayed complications such as granuloma formation11,13,15, suture
infection11,13,17, sling exposure8,11 or hypertro-phied
scar formation12. This is in contrast to other researchers who have
experienced all such complica-tions with different sling materials. An
important aspect to look for is that all these above mentioned complications
were somehow related to the sling materials and not the surgical technique or
expertise.
CONCLUSION
Frontalis suspension is an effective procedure for the cure of
unilateral ptosis with poor levator function. Cosmetically acceptable symmetry
in primary position can be achieved by addressing only the affected eye rather
than operating both eyes including the normal eye. It is not associated with
any serious complication. It shows promising long term results without any
significant cosmetic decline.
Author’s Affiliation
Dr. S. Hassan Raza Jafri
Assistant Professor
Isra Postgraduate Institute of
Ophthalmology
Al-Ibrahim Eye Hospital, Karachi
Dr. Abdul Rauf
Senior Registrar
Isra Postgraduate Institute of
Ophthalmology
Al-Ibrahim Eye Hospital, Karachi
Dr. Nazia Qidwai
Postgraduate Resident
Isra Postgraduate Institute of
Ophthalmology
Al-Ibrahim Eye Hospital, Karachi
Dr. Abdul Rashid Shaikh
Assistant Professor
Isra Postgraduate Institute of
Ophthalmology
Al-Ibrahim Eye Hospital, Karachi
Dr. Fayaz Ahmed Soomro
Senior Registrar
Isra Postgraduate Institute of
Ophthalmology
Al-Ibrahim Eye Hospital, Karachi
Dr. Ashraf Dawood
Senior Registrar
Isra Postgraduate Institute of
Ophthalmology
Al-Ibrahim Eye Hospital, Karachi
REFERENCES
1.
Collins
JRO. Ptosis. In: A
manual of systemic eyelid surgery. 2nd ed.
2.
Kanski JJ.
Eyelids. In: Clinical ophthalmology. 6th ed.
3.
Mehmood H. Levator
resection in congenital ptosis with poor levator function. Pak J Ophthalmol
1997; 13:103-106.
4.
Holds JB, McLeish WM, Anderson RL. Whitnall’s
sling with superior tarsectomy for the correction of severe unilateral
blepharoptosis. Arch Ophthalmol 1993; 111: 1285-91.
5.
Kanski JJ.
Eyelids. In: Clinical ophthalmology. 6th ed.
6.
Agarwal
S. Lids, Adenexa and Orbit. In: Textbook of
Ophthalmology. 1stedition.
7.
Callahan
A. Correction of unilateral blepharoptosis with bilateral
eye suspension. Am J Ophthalmol. 1972; 74, 321.
8.
Kersten RC, Bernardini FP, Khouri L, Moin M,
Roumeliotis
AA, Kulwin DR.
Unilateral
frontalis sling for the surgical correction of poor-function ptosis. Ophthal. Plast Reconstr Surg. 2005;
412-6.
9.
Chong
KK, Fan DS, Lai CH, Rao SK, Lan PT, Lam DS. Unilateral ptosis
correction with mersilene mesh frontalis sling in infants: thirteen year
follow-up report. Eye 2010, 44–9.
10. Junceda-Moreno J, Saurez-saurez E,
Dos-Santos-Bernardo V.
Treatment of palpebral ptosis with frontal suspension: a comparative study of
different materials. Arch Soc Esp Oftalmol. 2005; 80: 457-61.
11.
Ben
Simon G, Macedo AA, Schwarcz RM, Wang DY, McCann JP, Goldberg RA. Frontalis suspension for upper eyelid
ptosis; evaluation of different surgical designs and suture material. Am J
Ophthalmol. 2005; 140: 877-85.
12.
Steinkogler FJ, Kuchar A, Huber E, Arocker-mettinger
E. Goretex soft
tissues patch frontalis suspension technique in congenital ptosis and in
blepharophimosis- ptosis syndrome. Plast Reconstr Surg. 1993; 92: 1057-60.
13.
Mencia – Gutierrez E, Clariana-Martin A, Gutierrez – Diaz
E, Monsalve-Cordova J, Isquiredo-Rodriguez C. Results and complications of expanded
polytetrafluoroethylene in frontalis suspension ptosis surgery. Study of 59
cases. Arch Soc Esp Oftalmol. 2005; 80: 443-8.
14.
Bajaj
MS, Sastry SS, Ghose S, Betharia SM, Pushker N. Evaluation of polytetrafluoroethylene
suture for frontalis suspension as compared with polybutylate-coated braided
polyester. Clin Experiment Ophthalmol. 2004; 32: 415-9.
15.
Wasserman
BN, Sprunger DT, Helveston EM.
Comparison of materials used in frontalis suspension. Arch Ophthalmol 2001;
119: 687-91.
16. Jafri HR, Nazia Q. Use of polypropylene suture as sling
material in frontalis brow suspension for congenital ptosis with poor levator
function. Ophthalmology update 2010; 8:15-18.
17.
Collins
JRO. Ptosis. In:
A manual of systemic eyelid surgery. 2nd ed.
18. Lee
V, Konrad H, Bruce C, Collin JRO. Etiology and
surgical treatment of childhood blepharoptosis. Br J Ophthalmol 2002; 86:
1282-86.