Original Article
Non-penetrating
Eye Injuries in Victims of Bomb Blasts and Mine Blasts
Mumtaz Alam, Mustafa Iqbal
Pak J Ophthalmol 2013, Vol. 29 No. 1
. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. .
.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
|
See end of
article for authors
affiliations …..……………………….. Correspondence
to: Mumtaz Alam House No 310, Street No 5, Sector E-4, Phase 7
Hayatabad, Peshawar. …..……………………….. |
Purpose: To study the type of non-penetrating eye
injuries in victims of bomb blasts and mine blasts and to assess their visual
outcome. Material and Methods: The study was
conducted at the Department of Ophthalmology, Khyber Teaching Hospital and
Iqbal Eye clinic Peshawar, from March 2010 to February 2012. Detailed history
was taken from all patients and complete ocular examination was done. In eyes
with poor or no view of fundus a B-scan ultrasonography was done. Management
and follow up varied according to the type and extent of eye injury. All the
relevant data was recorded on a proforma. Results: Total number of
patients was 52, including 50 males (96.15%) and 02 female (03.84%). Mean age
of patients was 24.12 years. Ocular injury was unilateral in 36 patients
(69.23%) and bilateral in 16 eyes (30.76%). Vitreous hemorrhage was the most
common ocular finding, seen in 21 eyes (30.88%). Conservative management was
done in 57 eyes (83.82%), while 11 eyes (16.17%) required surgical
intervention. Visual acuity improved in 49 eyes (72.05%) and remained
unchanged in 19 eyes (27.94%). Final best corrected visual acuity was 6/12 or
better in 40 eyes (58.82%). Conclusion: Visual prognosis of
non-penetrating eye injuries in blast victims is usually good. Most cases do
not require surgical intervention and can be managed conservatively. |
Ocular
injury is an important cause of monocular visual impairment and blindness in
younger age group1,2. Approximately 2 million eye injuries occur in
the United States every year; and more than forty thousand result in permanent
visual impairment3.
Ocular injuries can be broadly divided into 2 groups i.e. closed
globe (without full-thickness wound of eye wall) and open globe (with
full-thickness wound of eye wall). Open globe injuries are divided into rupture
and laceration. Closed globe injuries are divided into contusion and lamellar
laceration4.
Bomb blast injuries are one of the most common causes of severe
ocular injury among adult males5. In our part of the world, blast
related eye injuries are becoming increasingly common. Bomb blast causes
peppering of the eye with multiple minute particles, which may be a combination
of plastic or metallic particles, gunpowder, sand, dust and organic debris6.
Closed globe eye injuries are common in blast victims and are
caused by the primary blast effect shock waves. The blast wave displaces a
dense medium across a less dense interface, and inertial forces may cause
displacement of optical structures causing non-penetrating eye injuries7.
The spectrum of eye injuries in blast victims ranges from very
mild non-sight threatening to extremely serious with potentially blinding cones-quences.
Our aim was to study the type of non-penetrating eye injuries in victims of
bomb blasts and mine blasts and to assess their visual outcome.
MATERIAL
AND METHODS
This was a prospective study conducted at Ophthalmology Department
of Khyber Teaching Hospital and Iqbal Eye Clinic Peshawar, from March 2010 to
February 2012. The study was done in collaboration with an organization, which
was working for people suffering war injuries. All the patients had bomb blast
or mine blast injuries. The patients were assessed by a trauma surgeon and any
serious injuries were properly managed. Patients were then referred to us for
the management of ocular injuries. All patients with closed globe injuries were
included in this study (68 eyes of 52 patients). Patients who had intraocular
foreign bodies (detected on clinical examination or CT scan) were excluded from
the study.
Informed consent was taken from all the patients. Detailed history
was taken and complete ocular examination was done including assessment of best
corrected visual acuity (BCVA) using Snellen visual acuity chart, pupillary
reaction, measurement of intraocular pressure with Perkin’s tonometer MK2
(Clement Clarke, London), anterior segment examination with slit-lamp (Takagi
SM-70, Japan) and dilated fundus examination with indirect ophthalmoscope
(Neitz, Japan) and/or with slit-lamp using 90D lens (Volk, USA). In eyes with
poor or no view of fundus a B-scan ultrasonography was done with AB 5500+ A/B
Scan (Sonomed, USA). Management and follow up varied according to the type and
extent of eye injury. All the relevant data was recorded on a performa.
RESULTS
The study included 68 eyes of 52 patients. Out of 52 patients, 50
were male (96.15%) and 02 female (03.84%). Mean age was 24.12 years (Range 04
to 65 years). Ocular injury was unilateral in 36 patients (69.23%) and
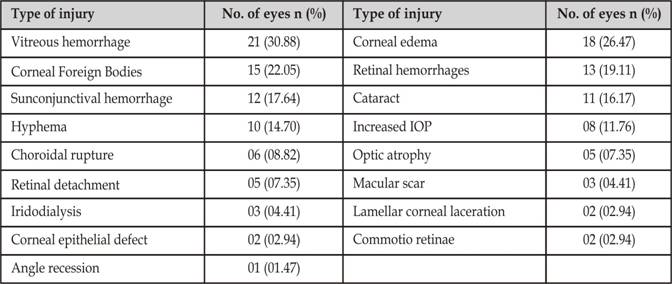
bilateral in 16 patients (30.76%). Vitreous hemorrhage was the most common
ocular finding, seen in 21 eyes (30.88%). Cataract was present in 11 eyes
(16.17%) and retinal detachment in 05 eyes (07.35%). The types of eye injuries
noted in our patients are given in Table 1. The treatment varied according to
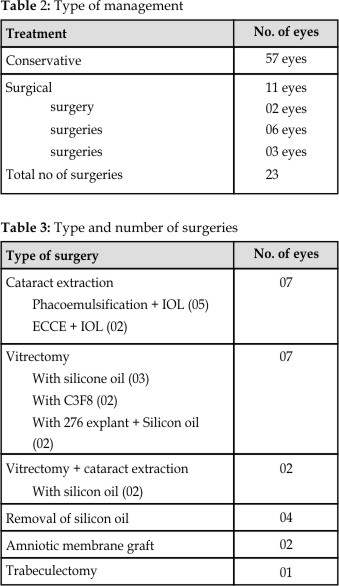
the type and severity of eye injury. Conservative management was done in 57
eyes (83.82%), while 11 eyes (16.17%) required surgical intervention Table 2.
Cataract extraction with intraocular lens implantation and pars plana
vitrectomy were the most commonly performed surgical procedures i.e. in 07 eyes
(10.29%) each. Vitrectomy was required in patients who had non-resolving
vitreous hemorrhage, or retinal detachment. The type and number of surgeries
are given in Table 3. In addition, 360 argon laser was done in 06 eyes (08.82%)
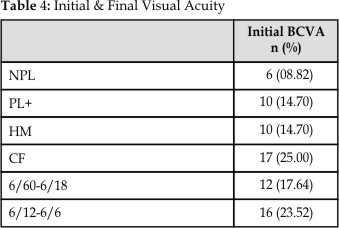
and YAG laser capsulotomy was done in 2 eyes (02.94%). Visual acuity improved
in 49 eyes (72.05%) and remained unchanged in 19 eyes (27.94%). 40 eyes
(58.82%) achieved best corrected visual acuity 6/12 or better. The initial and
final visual acuities are given in Table 4.
DISCUSSION
Trauma is a common cause of ocular morbidity. The effect of trauma
may be apparent immediately or may
develop later as a secondary complication. Ocular trauma can cause
permanent visual or cosmetic defect in the affected individuals and is one of
the major cause of monocular blindness and impaired vision throughout the world8.
In addition to the impact on affected individuals, blindness and
severe visual impairment resulting from the injuries have important
socioeconomic implications. The cost of treatment including hospital stay is
tremendously high, whereas, the indirect cost resulting from loss of
productivity by young men is equally important9. Developing
countries carry the largest burden of such accidents, but are the least able to
afford the costs10,11.
Bomb blast and mine blast are becoming increasingly common causes
of ocular injuries, especially in this part of the world. In a study of 387
randomly selected soldiers injured by blasts in Iraq, 329 (89%) sustained
ocular injuries12-14. In the study of Mader TH et al,15
36.3% of all ocular injuries were closed globe, while in the study of Weichel
ED et al16 54.16% of all eye injuries were closed globe injuries.
Vitreous hemorrhage was the most common ocular finding, seen in 21
eyes (30.88%), followed by corneal edema, seen in 18 eyes (26.47%), corneal
foreign bodies in 15 eyes (22.05%), retinal hemorrhages in 13 eyes (19.11%) and
subconjunctival hemorrhage in 12 eyes (17.64%). Cataract was present in 11 eyes
(16.17%) and retinal detachment in 05 eyes (07.35%). Most of the eyes (83.16%)
were managed conservatively, only 11 eyes (16.17%) required surgical
intervention. Cataract, vitreous hemorrhage and retinal detachment were the most common indications for
surgical intervention.
Visual outcome and prognosis in patients with ocular trauma due to
blasts, depends upon the type of injury sustained. Majority of the patients
with perforating injuries have poor visual outcome. Closed globe injuries
usually have better visual outcome as compared to open globe injuries16.
In our study, the best corrected visual acuity (BCVA) improved in
49 eyes (72.05%) and remained unchanged in 19 eyes (27.94%). 40 eyes (58.82%)
had final BCVA > 6/12 or better, in 10 eyes (14.70%) the BCVA was ranging
from 6/60 to 6/18 and in 18 eyes (26.47%) it was < 6/60. In the study of
Weichel ED et al,16 42 % of all eyes (including both open globe and
closed globe injuries) achieved a BCVA of 6/12 or better, closed – globe
injuries accounted for 65% of BCVA of 6/12 or better.
CONCLUSION
Bomb blast is becoming increasingly common cause of ocular
injuries. Visual prognosis of non-penetrating eye injuries in blast victims is
usually good. Most cases do not require surgical intervention and can be
managed conservatively.
Author’s Affiliation
Dr. Mumtaz Alam
Senior Registrar
Ophthalmology Department
Kuwait
Teaching Hospital, Peshawar
Dr. Mustafa Iqbal
Professor & In charge Eye “B” Unit
Khyber Teaching Hospital, Peshawar
REFERENCES
1.
Hasnain
SQ, Kirmani M. A 5 year retrospective case study of
penetrating ocular trauma at the
2.
Khattak
MN, Khan MD, Muhammad S, Mulk RA. Untreatable
monocular blindness in Pakistani eye patients. Pak J Ophthalmol 1992; 8: 3-5.
3.
McGwin
G, Xie A, Owsley C. The rate of eye injury in the
4.
Kuhn F,
Morris R,
Witherspoon
CD, Mester V.
The Birmingham
Eye Trauma Terminology system (BETT). J Fr Ophtalmol. 2004; 27:
206-10.
5.
Newmann
TL, Russo PA. Ocular sequelae of BB injuries to eye and
surrounding adnexa. J Am Optom Assoc. 1998; 69: 583-90.
6.
Jackson
H. Severe ocular trauma due to landmines and other
weapons in
7.
Harlan
JB, Pieramici DJ. Evaluation of patients with ocular
trauma. Ophthalmol Clin North Am. 2002; 15: 153-61.
8.
Jackson H. Bilateral blindness due to trauma in
9.
Baig
MSA, Zafar MU, Anwar M, Rab M, Khokar AR. Major
ocular trauma. (An analysis of 98 admitted cases). Pak J Ophthalmol. 2004; 20:
148-52.
10. Umeh RE,
11. Ilsar M, Chirambo M, Belkin M.
Ocular injuries in
12. Ramasamy A, Harrisson SE, Clasper
JC, Stewart MP. Injuries from roadside improvised
explosive devices. J Trauma. 2008; 65: 910-4.
13. Weichel ED, Coyler MH.
Combat ocular trauma and systemic injury. Curr Opin Ophthalmol. 2008; 19:
519-25.
14. Wolf SJ, Bebarta MV, Bonnet CJ.
Blast injuries. Lancet 2009; 374: 405-15.
15. Mader
TH,
16.
Weichel ED, Colyer MH,