Original Article
Correlation between Axial Length and Retinal Nerve Fiber
Layer Thickness in Myopic Eyes
Muhammad Abdul Rehman Akram, Irfan Qayyum
Malik, Idress Ahmad, Suhail Sarwar, Mumtaz Hussain
Pak J Ophthalmol 2013, Vol. 29 No. 3
. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. .
.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
|
See end of article for authors affiliations …..……………………….. Correspondence to: Abdul Rehman Akram Ophthalmology Department Mayo Hospital Lahore …..……………………….. |
Purpose: To determine the correlation between axial length and retinal
nerve fiber layer thickness in myopic eyes. Material and method: One hundred patients of myopia with best corrected visual acuity
of at least 6/12 in the best eye were included in this study. Optical
coherence tomography was done with dilated pupils. Axial length was measured
with A-Scan. After pupillary dilation, retinal nerve fiber layer thickness
was measured with optical coherence tomography (OCT) around the center of
optic disc. Mean retinal nerve fiber layer thickness was generated by
automated computerized program in the analysis report and compared with the
built in age-matched normative database in 3D OCT. Results: The mean age was 27.08 + 7.85 years. There were 50 males (50%)
and 50 (50%) females. The mean spherical equivalent (myopia) was -2.95 D +
1.36. The mean axial length 23.92 + 0.614. The mean retinal nerve fiber layer
(RNFL) thickness was 111.49 µm + 4.04. Pearson coefficient of correlation was
-.328. Conclusion; In myopic patients the RNFL thickness decreases with increasing
axial length. |
Myopia is the most common ocular abnormality worldwide. Its exact
prevalence in Pakistan is not known but different studies showed different
results1,2 in the different areas of Pakistan. Retinal changes in
persons with high myopia include peripapillary atrophy, peripheral lattice
degeneration, tilting of the optic disc, posterior staphyloma and breaks in
Bruch’s membrane.
Although retinal nerve fiber layer thinning is indicative of
glaucomatous damage, it remains uncertain whether retinal nerve fiber layer
thickness would vary with the refractive status of the eye). It is
therefore important to investigate whether any correlation exists between
retinal nerve fiber layer thickness and axial length in myopia. For every 1 mm
greater axial length, mean retinal nerve fiber layer thickness decreases by
approximately 2.2 µm.3
The aim of this study is very important because it measures
retinal nerve fiber layer thickness changes with the increase in axial length
as in myopia. The decreasing retinal nerve fiber layer thickness is a major
risk factor to develop glaucoma which is a second most common cause of
blindness worldwide.4
MATERIAL AND METHODS
100 patients fulfilling the inclusion criteria were taken from the
outdoor clinic of institute of ophthalmology Mayo hospital, Lahore. Informed
consent, socio-demographic data (name, age, gender, address and contact
number), past medical and surgical history were recorded. The study was
conducted in accordance with ethical standards approved by the hospital
committee. Examination included visual acuity with Snellen’s chart, refractive
error with auto-refractometer, slit lamp examination for anterior segment
evaluation, indirect ophthalmoscopy using 20 D lens for fundus examination with
dilated pupils.
Axial length was measured with A-Scan. After pupillary dilation,
retinal nerve fiber layer thickness was measured with OCT around the center of
optic disc. Mean retinal nerve fiber layer thickness was generated by automated
computerized program in the analysis report and compared with the built in
age-matched normative database in 3D OCT (Topcon 3D OCT-1000). To control the biases, only one expert person
recorded the axial length and retinal nerve fiber layer thickness. The side of
the eye was selected randomly. All the
required information was collected on an especially designed proforma (attached
herewith).
RESULTS
One hundred eyes of 100 patients were included in the study among
which 60 (60%) were right eyes and 40 (40%) were left eyes (table 3). The mean
age was 27.08 ± 7.85 years (table 2). There were 50 males (50%) and 50 (50%)
females (table I). We studied the effect of axial myopia according to the axial
length of the patient on the thickness of retinal nerve fiber layer. The mean
spherical equivalent of the myopic patients was -2.95 D ± 1.36 (Table 4). The
mean axial length was 23.92 ± 0.614. The mean retinal nerve fiber layer (RNFL)
thickness was 111.49µm ± 4.04
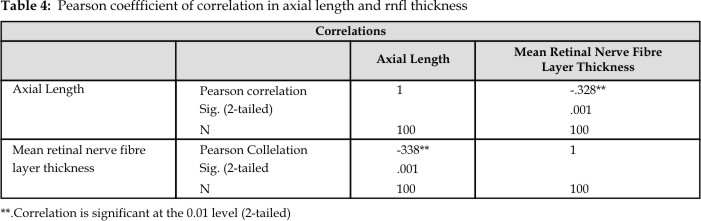
Axial myopia is related with increased axial length and it affects
the thickness of RNFL. In our study we calculated the Pearson’s coefficient
correlation between axial length and RNFL thickness by using SPSS and it was
-.328 which is significant at the level of 0.01 The p value was 0.001 which is
highly significant. Pearson coefficient of correlation (r) between axial length
and retinal nerve fiber layer thickness was calculated - 0.314 in myopic eyes in my reference study. For every 1 mm
greater axial length, mean retinal nerve fiber layer thickness decreases by
approximately 2.2µm.
Table
1: Distribution of cases by spherical equivalent
(Myopia) (n = 100)
|
Total no. of patients |
100 |
|
Mean |
-2.96 |
|
Standard Deviation |
± 1.36 |
The results of our study show that given parameters in different
population groups regarding axial length and RNFL thickness are also valid for
our population which we are dealing in Mayo Hospital. So RNFL thickness values
can be used in our population for early glaucoma detection and monitoring.
Table
2: Distribution of cases by axial length (n = 100)
|
Total no. of patients |
100 |
|
Mean |
23.92 |
|
Standard Deviation |
± 0.61 |
Table
3: Distribution of cases by rnfl thickness
(n =100)
|
Total no. of patients |
100 |
|
Mean |
111.49 |
|
Standard Deviation |
± 4.04 |
DISCUSSION
Retinal nerve fiber layer damage invariably occurs in
glaucoma.5 Various investigational modalities like, retinal nerve
fiber layer analyzer (NFA), scanning laser ophthalmoscope (GDx, and GDx with
variable corneal compensation), and OCT are used to measure the RNFL changes. OCT is a non-invasive, non-contact modality
that can be used for measurement of peripapillary RNFL thickness. It is found
to correlate with RNFL as measured with scanning laser ophthalmoscope (SLO) and
the Heidelberg retinal tomography (HRT).6 OCT measured RNFL thickness is not
affected by the corneal and lenticular birefringence, as is the case with
confocal scanning laser polarimetry. No additional reference plane
is required to calculate the RNFL thickness because OCT provides an absolute
cross-sectional measurement of retina, from which RNFL thickness is calculated.
A high level of correlation between OCT generated RNFL thickness
and visual function has been reported in previous studies. The RNFL may show a racial variation and the various values may
be specific to the population under study. The detection of RNFL loss also
varies in accordance with the imaging technology used, and the normative RNFL data
of the concerned population. RNFL thickness parameters are already studied in
the western population7.
This
study is important as no study is available for Pakistani population which
gives a normal data of RNFL thickness which can be used as reference in
different diseases especially glaucoma in which there is loss of RNFL which can
be compared with the age match control of normal population.8
The mean RNFL thickness in our sample population was 113.91
microns, and it is comparable to the RNFL thickness reported in the Chinese
population9. A summary of some of the previous reports
on normal RNFL thickness parameters is presented in reference studies. It shows a higher value of RNFL thickness in most of the studies
in Caucasians (except those 1 reported by Bowd and
Mistelberger when
compared to Chinese eyes. Such a discrepancy has not been addressed earlier but
might be related to the ethnicity of study group, or to the OCT model, and the
analysis protocol used. Although retinal nerve fiber layer thinning is
indicative of glaucomatous damage, it remains uncertain whether retinal nerve
fiber layer thickness would vary with the refractive status of the eye. In a
study held at Hong Kong eye hospital, Pearson coefficient of correlation (r)
between axial length and retinal nerve fiber layer thickness was calculated -
0.314 in myopic eyes10. For every 1 mm greater axial length, mean
retinal nerve fiber layer thickness decreases by approximately 2.2 µm.11
The
thinning of RNFL is a very good indicator of glaucoma but it also occurs in
myopic eyes, it means measuring RNFL thickness without knowing refractive
status can lead to misdiagnosis of glaucoma. We have found the relation between
increased axial length and RNFL in our population, which is almost the same as
concluded in others studies in the world. This fact has enabled us to use RNFL
parameter for glaucoma detection in myopic eyes effectively.12
There
was no effect of gender on the RNFL parameters measured in our study. A similar
finding has been reported previously.13 Schuman et al showed nerve fiber layer of men were
usually thinner than the females, but not statistically significant.14
CONCLUSION
In conclusion, our study provides a reliable correlation values
between axial length and retinal nerve fiber layer thickness in myopic
Pakistani eyes by optical coherence tomography. This can serve as a useful
guideline in diagnosis, management and research in glaucoma in myopic eyes.
Author’s Affiliation
Dr. Abdul Rehman Akram
Eye Unit-II
Mayo Hospital, Lahore
Dr. Irfan Qayyum
Eye Unit-II
Mayo Hospital, Lahore
Dr Idrees Ahmad
Assistant Professor
Sharif Medical College Lahore
Dr. Suhail Sarwar
Assistant Professor of
Ophthalmology
Eye Unit-III
Mayo Hospital, Lahore
Dr. Mumtaz Hussain
Professor of Ophthalmology
Eye Unit-II
Mayo Hospital, Lahore
REFERENCES
1.
Masood S, Hussain Z, Ahmad A, Tanveer ZH, Ahmad I. Incidence of myopia in school going children in Rahim Yar Khan Professional Med J.
2007; 14: 422-5.
2.
Alam H, Siddiqui I, Jafri
SI, Khan AS, Ahmed SI, Jafar M. Prevelance of refractive error in school
children of Karachi. J Pak Med Assoc.
2008; 58: 322-5.
3.
Budenz
DL, Anderson
DR, Varma
R. Determinants of normal
retinal nerve fiber layer thickness measured by Stratus OCT. Ophthalmology. 2007; 114:
1046-52.
4.
In focus: Glaucoma is second leading cause of
blindness globally. Bull World Health Organ. 2004; 82: 887.
5.
Soliman MA, Van Den Berg
TJ, Ismaiel AA, Dejong
LA, De Smet MD. Retinal nerve fibre layer analysis; relationship
between optical coherence tomography and red free photography. Am J Ophthalmol.
2002; 133: 187-95.
6.
Patker HM, Schuman JS,
Hertzmerk E. Optical coherence tomography of the retinal nerve fiber layer,
with comparison to Heidelberg retinal tomography optic nerve head measurements,
in normal and glaucomatous human eyes. In Lemji Hg, Schuman JS, editors. The
shape of Glaucoma. Quantitative Neural Imaging Techniques. The Hague: Kugler
Publications. 2000; 149-84.
7.
Bowd C, Weinreb RN, Williams JM, Zangwill LM. Retinal nerve fiber layer thickness in ocular hypertensive,
normal and glaucomatous eyes with optical coherence tomography. Arch Ophthalmol.
2007; 118: 22-26.
8.
Araie
M, Arai
M, Koseki
N, Suzuki
Y. Influence of myopic refraction on visual
field defects in normal tension and primary open angle glaucoma. Jpn J
Ophthalmol. 1995;
39: 60-4.
9.
Liu X, Ling Y, Zhou W,
Zheng X, Liang D. Qualitative and quantitative measurement of retinal nerve fiber
layer in primary open angle glaucoma by optical coherence tomography. Honghua
Yan Ke Za Zhi. 2006; 36: 420-8.
10.
Leung CK, Mohammad S, Leung
KS, Cheung CY, Chan SL, Cheng DK, Lee AK, Leung GY, Rao SK, Lam DS. Retinal nerve fiber layer measurements in myopia: An optical
coherence tomography study. Invest Ophthalmol Vis Sci. 2006; 47: 5171-6.
11.
Budenz
DL, Anderson DR, Varma R, Schuman J, Cantor L, Savell J, Greenfield DS, Patella VM, Quigley HA, Tielsch J. Determinants of normal retinal nerve fiber layer
thickness measured by stratus OCT. Ophthalmology 2007; 11:1046-52.
12.
Shoji T, Sato H, Ishida M, Takeuchi M, Chihara E. Assessment
of glaucomatous changes in subjects with high myopia using spectral domain
optical coherence tomography. Invest Ophthalmol Vis Sci. 2011; 52: 1098-22.
13.
Guedes V, Schuman JS,
Hertzmerk E, Wollstein G, Correnti A, Mancini R, Lederer D, Voskanian S, Velazquez L, Pakter HM, Pedut-Kloizman T, Fujimoto JG, Mattox C. Optical coherence tomography measurement of macular and nerve
fiber layer thickness in normal and glaucomatous eyes. Ophthalmology. 2003; 110:
177-89.
14.
Schuman JS, Hee MR,
Puliafito CA, Wong C, Pedut-Kloizman T, Lin CP, Hertzmark E, Izatt JA, Swanson EA, Fujimoto JG. Quantification of nerve fibre layer thickness in normal and
glaucomatous eyes using optical coherence tomography. Arch Ophthalmol. 1995; 113:
586-96.