PPV was developed by
Robert Machemer, and it was performed using a 14-gauge instrument (2.1-mm
diameter). 20G vitrectomy remained in vogue in the last two decades of the 20th
century. Peyman developed a 23-G PPV probe in 19901, primarily for vitreous
and retinal biopsy. Hilton also described an office-based sutureless-vitrectomy
system. Fujii and associates2,3,
modified vitrectomy instruments and introduced 25-G PPV with sutureless
self-sealing sclerotomies. Reduction in postoperative discomfort along with
short surgical and recovery time, are few advantages of 23G over 20G PPV4-7.
The 23-G PPV induces no corneal astigmatism and there
is very significant stability for all the measured parameters between the
preoperative and the postoperative conditions8,9. The self-sealing sclero-tomies
and the sutureless scleral and conjunctival incisions explain the corneal
curvature stability after the procedure. By contrast, the conventional 20-gauge
vitrectomy is responsible for significant corneal topographic changes in the
first preoperative days or weeks10.
The purpose of the
study was to compare the pre-operative and post-operative corneal astigmatism
and hence assess corneal stability in 20G sutured versus 23G sutureless
vitrectomy.
MATERIAL AND
METHODS
The study was
carried out at
There were 40
eyes included in this study and 20 each were assigned to 20G & 23G group.
Sampling technique was a comparative, consecutive and interventional study. Patients were selected randomly in
both groups. Those included in the study had epiretinal membranes (ERM),
macular hole, non-clearing vitreous hemorrhage, retained lens fragments,
vitreomacular traction, diabetic
macular edema and tractional retinal detachment (TRD). The patients who required cataract surgery
per operatively or had a corneal pathology were excluded. Patients who required relaxing incisions to cornea,
removal of intra-ocular foreign body, repair of rhegmatogenous retinal
detachment or silicone oil insertion
were also excluded from the study.
Forty consecutive
eyes of patients presenting in vitreo-retina out-patient department of the
Institute of Ophthalmology, Mayo Hospital, Lahore, from 1st January
2011 to 31st March were included in our study. Examination of the
eyes included the recordings of corneal astigmatism, keratometric readings
[M2], slit-lamp examination of anterior segment, fundus examination, B scan,
OCT and FFA if required. All
data including preoperative, operative and post operative recordings were
collected. Follow up period was
extended over 3 months with visits on day 1, 7, 30, 60 and 90. Outcome
variables included preoperative and post-operative corneal keratometric
readings (astigmatism) on each follow-up visit. Data was entered and analyzed
using computer program EPI Info version “10” to find out frequencies and
percentages. Descriptive statistics ware applied to determine the mean and
standard deviation (SD) for variables like keratometric readings and hypotony.
Chi-square test was applied to evaluate the results. P-value ≤0.05 was
considered significant.
RESULTS
In
20G group 11 were males and 9 were females whereas in 23G group 10 were males
and 10 females. In 20G group 14 had vitreous haemorrhage, 2 had macular hole
and 4 had dropped lens in the vitreous whereas in 23-g group 10 had vitreous
haemorrhage, 9 had macular hole and 1 had ERM (Macular Pucker).
Posterior
vitreous detachment (PVD) had to be created intra-operatively in 10 (50%) of 20
eyes in the 23G group and 6 (30%) of 20 eyes in the 20G group. Retinal breaks
associated with the maneuvers performed to create a PVD occurred in 1 (10%) of
10, and 1 (16.6%) of 6 eyes in the 23G and 20G groups, respectively, and were
treated effectively with photocoagulation intra-operatively. No retinal
detachments developed.
No
severe postoperative hypotony developed in either group, although in 23G
group-1 eye had IOP less than 7 mm Hg 1stday postoperatively which
increased to more than 10-mm Hg in 2 days and no surgical intervention was
required. There was no significant difference in complications in either group
preoperatively and postoperatively. No choroidal detachment or bacterial
endophthalmitis developed in either group.
The
corneal induced astigmatism was lower 1 week postoperatively in the 23G group (P=.006) as compared with the 20G group (P
= .001). One month postoperatively, the surgically induced corneal astig-matism
was still lower in the 23-gauge group (P = .01).
Astigmatism in
20G group on first day had ranged from 2.5 D to 3.5 D with a mean of 3.25D,
which reduced to a mean of 2 D on the 7th post operative day, 1.25 D
after one month, 0.75 D by 2 months and 0.5 to 0.6 D by 3 months whereas
astigmatism in 23G group on 1st post-operative day ranged from 0.25
D to 0.75 D with mean of 0.6 D, 0.5 D on 7th post operative day, 0.4
D after 1 month, 0.3 D after 2 months and 0.25 D after 3 months.
DISCUSSION
In our study there had been very
rapid improvement and very low surgically induced astigmatism one week after
surgery in patients undergoing 23-G PPV as compared with those undergoing 20-G
PPV. Less surgically induced astigmatism in patients who underwent 23-G PPV had
earlier visual rehabilitation with maximum vision improvement in the first
couple of weeks. Although much work has been done on 25-G PPV and its role in
surgically induced astigmatism, only limited studies are available regarding
surgically induced astigmatism in 20-G and especially 23-G PPV. Our study shows
that in the early post-operative period, 23-G trans-conjunctival surgery is
comparable to 25-G PPV with much less post-operative astigmatism, proving these
techniques to be superior to the 20-G PPV. Complications, although occasionally
common with 20-G PPV, were not observed in patients undergoing 23-G PPV. A
patient had post-operative hypotony and a couple of patients had flare in
anterior chamber after 23-G PPV, who recovered early with treatment.
Fig. 1:
- Indications for 20 G PPV
Fig. 2:
- Indications for 23 G PPV
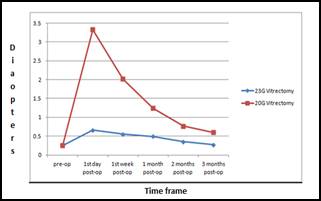
Graph: Surgically
induced corneal astigmatism in 23G and 20G PPV
and associates described that the
induced astigmatism in patients undergoing 20-guage vitrectomy, usually
transient, may be attributed to suturing at the entry ports. Slusher
et al reported that the lysis of the sutures after PPV reduce postoperative
corneal astigmatism by more than 5.0 D. Bergmann et al reported that scleral
cautery near the incisions changed corneal curvature by causing thermal
contracture of the treated tissue and immediate central steepening.
Wimpissinger and associates who compared the sutureless 23-G system with the
standard 20-G system in PPV for various vitreoretinal disorders, randomly
divided 60 patients into 2 groups and reported that the opening and closure
times were significantly shorter and the duration of the vitrectomy was
significantly longer in the 23-gauge system compared with the 20-gauge
vitrectomy group. However, the degree of retinal manipulation and the overall
duration of surgery did not differ significantly between the groups. Vitreous
surgery for pre-retinal membranes can be a good indication for using the
sutureless-trans-conjunctival 23G system to capitalize on the merits of and
decrease the disadvantages of the surgical system.
CONCLUSION
The 23-gauge procedure resulted in less
corneal astigmatic changes as compared to conventional 20-gauge vitrectomy.
Author’s Affiliation
Dr.
Syed Raza Ali Shah
Associate Professor King Edward Medical
University/ Mayo Hospital Lahore, VR Fellow, College of Ophthalmology and
Allied Visual Sciences Institute of Ophthalmology
Dr.
Tehseen Mehmood Mahju
Senior Registrar and VR Fellow College of
Ophthalmology and Allied Visual Sciences, Institute of Ophthalmology, King
Edward Medical University / Mayo Hospital Lahore
Dr.
Qasim Lateef Chaudry
Assistant
Professor College of Ophthalmology and Allied Visual Sciences Institute
of Ophthalmology, King Edward Medical University / Mayo Hospital Lahore
Prof.
Asad Aslam Khan
Professor of Ophthalmology, King Edward
Medical University / Mayo Hospital Lahore, Director General College of
Ophthalmology and Allied Visual Sciences Institute of Ophthalmology
Dr.
Chaudry Nasir Ahmad
Assistant Professor College of
Ophthalmology and Allied Visual Sciences Institute of Ophthalmology, King
Edward Medical University / Mayo Hospital Lahore
Ms.
Zoya Raza
Statistical Analyst
Lahore School of Economics, Lahore
REFERENCES
1.
2.
Fujii GY, De Juan Jr E, Humayun MS, Chang TS, Pieramici DJ, Barnes
A, et al. Initial experience using the
trans-conjunctival sutureless vitrectomy system for vitreoretinal surgery. Ophthalmology.
2002; 109:
1814-20.
3.
Fine HF, Iranmanesh R, Iturralde D, Spaide RF. Outcomes of 77 consecutive cases of 23-gauge trans-conjunctival
vitrectomy surgery for posterior segment disease. Ophthalmology 2007; 114:
1197-1200.
4.
Oshima Y, Ohji M, Tano Y.
Surgical outcomes of 25-gauge trans-conjunctival vitrectomy combined with
cataract surgery for vitreoretinal diseases. Ann Acad Med
5.
Lakhanpal RR, Humayun MS, de Juan Jr E, Lim JI, Chong LP, Chang TS
et al. utcomes of 140 consecutive cases
of 25-gauge trans-conjunctival surgery for posterior segment disease. Ophthalmology.
2005; 112:
817-24.
6.
Jackson
T. Modified sutureless sclerotomies in pars plana
vitrectomy. Am J Ophthalmol. 2000; 129: 116-7.
7.
Assi
AC, Scott RA, Charteris DG. Reversed self-sealing pars plana
sclerotomies. Retina. 2000; 20: 689-92.
8.
Domniz YY, Cahana M,
9.
.
Clinically significant corneal astigmatism and pars plana vitrectomy. Ophthalmic Surg Lasers. 2002; 33: 5-8.
10.
11. Hubschman JP, Gupta A,
Bourla DH, Culjat M, Yu F, Schwartz SD. 20, 23, and 25 gauge vitreous
cutters: performance and characteristics evaluation. Retina. 2008; 28: 249-57.
12. Wimpissinger
B, Kellner L, Brannath W, Krepler K, Stolba U, Mihalics C, Binder S. enty-three-gauge versus 20-gauge
system for pars plana vitrectomy: a prospective randomized clinical trial. Br J Ophthalmol. 2008; 92: 1483-7.