Lacrimal
drainage system obstruction may be present in approximately 50% of newborn
infants congenitally. Mostly obstructions opened spontaneously within 4 – 6
weeks after birth. The newborn with epiphora presented at 3 – 4 weeks of age,
mostly unilaterally and sometimes bilaterally. Approximately 90% resolved
within 1st year of life, with or without massaging or topical antibiotic drops.
If epiphora persisted, then probing and syringing was optional, non-invasive
treatment. But some children present again with epiphora and discharge. And the
next option remains the eternal DCR or the closed intubation. The aim of our
study was to avoid the external DCR and relief of symptoms of epiphora and
discharge with closed intubation in children up to 4 years of age.
MATERIAL AND METHODS
This was
an interventional retrospective hospital based study. Patients were selected
from the outpatient department of Mayo Hospital Lahore, KEMU. All 200 children
up to 4 years of age who have had failed probing and syringing once or twice
and presented with epiphora discharge and mucocele formation, were included in
this study. Patients were given general anaesthesia. After draping both the
puncti were dilated with punctum dilator. Then, probing and syringing was done
up to the level of inferior opening of nasolacrimal duct into the inferior
turbinate of the nose. Then Crawford Silicon Tube was passed through the same
anatomical passage. Tube is appreciated in the nose then pulled from the nose
with artery forceps. The same procedure was repeated from the upper punctum and
both ends of Crawford Silicon Tube were tied in the nose. Patient was
discharged on topical and systemic antibiotics and NSAIDs. Follow-Up was done
at the interval of 1 month, 3 months and 6 months. Then the tube was removed
under general anaesthesia after 6 to 8 months.
RESULTS
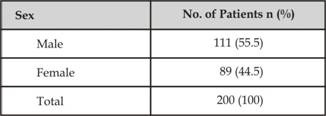
There were
111 (55.5%) male and 89 (44.5%) females. The age range was 1-4 years. Among
these, 89 (44.5%) were 1-2 years of age, 68 (34%) were 2-3 years of age, 43
(21.5%) were 3-4 years of age. Preoperatively all the children had epiphora and
discharge with failed probing and syringing once or twice. Postoperative
follow-up was done at the interval of 1 month, 3 months and 6 months, during
which 172 (86%) had no epiphora and discharge whereas 28 (14%) presented with
epiphora and discharge. Failure as compared to age presentation observed during
this period was as follows; 20 (71.4%) in 3-4 years of age; 6 (22.2%) in 2-3
years of age; 2 (7.4%) in 1-2 years of age. Complication noted with silicon
tube were, Cheese wiring of canaliculli and Pulling out of tubes.
Presenting age chart
Failure age ratio chart

Fig. 1: 1st post op day.

Fig. 2: After 3 Months.
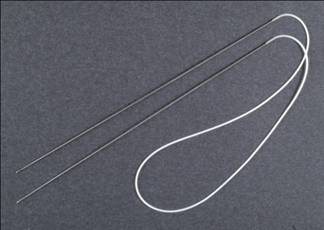
Fig. 3: Crawford tube with olive tip.
DISCUSSION
Congenital
naso-lacrimal duct obstruction is a common congenital anomaly even in full term
infants and is due to delay in the normal development of the
system. Neonates have tear secretion at birth and 96% to 98% have a totally
patent and functional drainage system at birth. The 2% to 4% who do not have an
intact lacrimal drainage system, have a thin residual membrane at the distal
end of the naso-lacrimal duct.
This membrane dissolves spontaneously in 80% to 90% of
infants within the first few months of life1, either spontaneously
or with medical treatment and massage2-3. The obstruction and the resultant
conti-nued tearing and discharge are not only unsightly and a potential source
of ocular infection, it also causes a lot of anxiety to young parents who are
inexperienced and apprehensive about their newborn babies4. In the
majority of cases, the cause of failure of conservative treatment is an
improper technique of lacrimal sac massage5. Surgical intervention
in the form of probing and irrigation of the naso-lacrimal duct is required in
the cases not responding to medical treatment and massage. We included the
epiphoric children in our study where probing and syringing didn't work at
least twice. The aim of our study was to avoid external DCR & relief of
symptoms of epiphora and discharge with closed intubation in children up to 4
years of age.in our study out of 200 patients 111 (55.5%) were male while 89
(44.5%) were females. The age range was 1 – 4 years. Among these, 89 (44.5%)
were 1 – 2 years of age, 68 (34%) were 2 – 3 years of age, 43 (21.5%) were 3 – 4
years of age. Preoperatively all the children had epiphora and discharge with
failed probing and syringing once or twice. Postoperative follow-up was done at
the interval of 1 month, 3 months and 6 months, during which 172 (86%) had no
epiphora and discharge whereas 28 (14%) presented with epiphora and discharge.
Failure to age ratio observed during this period was as follows; 20 (71.4%) in
3 – 4 years of age; 6 (22.2%) in 2 – 3 years of age; 2 (7.4%) in 1 – 2 years of
age.
Other complication noted with silicon tube were
1.
Cheese wiring of canaliculi
2.
Pulling out of tubes
Probing of the naso-lacrimal duct is the
first line of treatment. However probe failure increases with age and is known
to double every 6 months. For this reason and in cases of persistent epiphora,
a second probing two to four months later is advocated. In failed cases with
persistent epiphora and recurrent infection, it may be necessary to perform a
dacryocys-torhinostomy (DCR) or closed intubation. In our study we did closed
intubation in all cases with aiming to avoid the patients from major surgery of
DCR.
In our study the success rate was 86% which is almost
consistence with the studies done in the past. It is quiet safe and effective
and the results are almost identical to DCR surgery. And the main thing is that
there is no external scar.
CONCLUSION
Closed intubation with silicon tube is an
effective treatment modality for children with age between 1 to 4 years. And it
is also noted that as the age increases the failure rate increases.
Author’s Affiliation
Dr. Muhammad Abdul Rehman Akram
Medical Officer
Eye Department, Mayo Hospital
Lahore
Dr. Irfan Qayyum
Eye Department, Mayo Hospital
Lahore
Dr. Ali Zain Ul Abidin
Medical Officer
Eye Department, Mayo Hospital
Lahore
Dr. Najam Iqbal Ahmad
Senior Registrar
Eye Department, Mayo Hospital
Lahore
Dr. Javed Iqbal Chaudhry
Assistant Professor
Eye Department, Mayo Hospital
Lahore
Dr. Mumtaz Hussain
Professor of Ophthalmology
Eye Department, Mayo Hospital
Lahore
REFERENCES
1.
Petersem RA, Robb RM. The natural course of congenital obstruction
of the naso-lacrimal duct. J Pediat Ophthal Strabismus. 1978; 15: 246-50.
2.
Muhammad Z, Khan MD. Timing of Probing in Naso-lacrimal Duct
Obstruction in Infants and Children. Pak J Ophthalmol. 1994; 10: 82-4.
3.
Mehmood T. Watery eyes, Pak J Ophthalmol. (Editorial), 2006; 22:
58-9.
4.
Nasir J, Mohyuddin M, Bhatti SA. Non Massaging Management of Congenital and
Infantile Naso-lacrimal Duct Obstruction. Pak J Ophthalmol 2007; 23: 84-6.
5.
Khan N, Khan MN, Jan S, Mohammad S. Congenital Naso-lacrimal Duct Obstruction:
Presentation and Management. Pak J Ophthalmol. 2006; 22: 74-8.