Lightning injury can cause multi system damage
and often results in high mortality. The consequences of being struck by lightning depend on several factors
at the time of the incident. Important features are the type of stroke, the current
and its distribution, and the victim’s position and clothing1. Ocular
injuries like thermal keratopathy, uveitis, hyphaema, anterior and posterior
subcapsular cataract, lens dislocation have been reported2.
Posterior segment complications like vitreous hemorrhage, retinal edema and
haemorrhage, retinal detachment, vascular occlusion, choriodal rupture, macular
involvement in the form of cystoid macular edema and macular hole have been
documented. Lightning induced nystagmus, anisocoria, optic neuropathy, Horner's
syndrome and multiple cranial nerve palsies has been reported2-4.
We
report a rare case of ocular injury due to lightning strike involving both
anterior and posterior segments with good final visual outcome.
CASE
REPORT
A 30 – years old female presented with painless diminution of
vision in BE following a lightning strike one month back. She was struck by
lightning when she along with her two family members were sitting on the
veranda of their house while it was raining outside. The neighbour who
accompanied her gave the rest of the history. She was unaware of the incident.
All three became unconscious following a lightning strike on a coconut tree
situated near the house. The coconut tree was burnt out. All three were
admitted in hospital in unconscious state and treated conservatively. Among the
three one sustained skin burns around her necklace, her husband sustained a
fracture of right humerus, may be due to fall on ground. But these two did not
develop any ocular complaints. After seven days of the incident she complained of
blurring of vision and redness in both eyes. She was examined by an
ophthalmologist and diagnosed as bilateral uveitis and was treated with topical
steroids and cycloplegics. Systemic examination like pulse, BP and renal
function were normal. There was no skin or eyelid burns. She developed loss of
hearing in the left ear due to rupture of tympanic membrane.
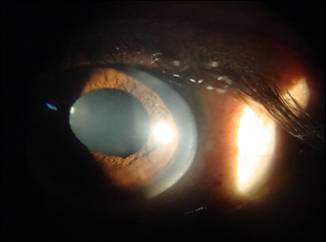
Fig. 1: Slit lamp photography showing Sphincter tear at 5’O Clock
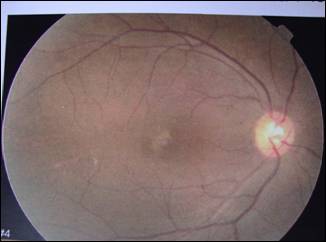
Fig. 2: Colour fundus picture showing RPE pigmentation.
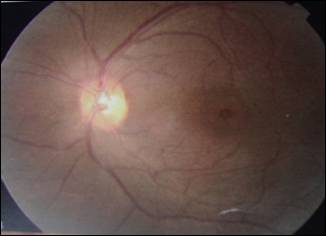
Fig. 3: Colour fundus picture
showing macula hole.
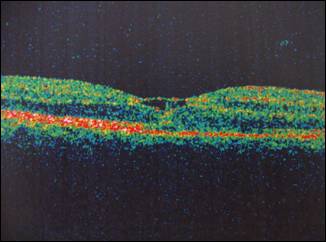
Fig. 4: OCT showing cystic changes in the macula
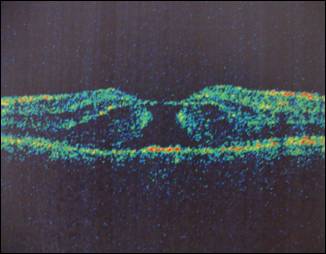
Fig. 5: Lightning induced
full thickness macular hole.
On
examination, her BCVA was 6/24 and 6/60 and intraocular pressure was 16 and 18
mm Hg respectively in RE and LE. Slit lamp examination revealed bilateral
resolving iridocyclitis, anisocoria (LE > RE) and sphincter tear at
5-0’clock position and anterior and posterior subcapsular cataract in both eyes
(LE > RE) (Fig. 1). Slit lamp biomicroscopy with a 90 D revealed
pigmentation of macula in RE (Fig. 2) and macular hole in LE (Fig. 3). The Watzke - Allen sign was positive in LE. OCT
revealed macular cyst in RE (Fig. 4) and a full thickness macular hole with a
thin bridging tissue over it in LE (Fig. 5). Non steroidal anti-inflammatory
drops were prescribed in both eyes for the uveitis.
The patient
reviewed with us 3 months later, when she had developed a total cataract in her
LE and advanced immature cataract in RE. Small incision cataract
surgery was done in BE. Post-operative BCVA was 6/9 in RE and 6/12 in LE.
Pigmentary changes were found in macular area of BE. The Watzke – Allen sign was negative in LE. We
assume that there was a spontaneous closure of the macular hole in LE but the
OCT could not be done because of patient’s unwillingness.
DISCUSSION
Lightning
is an uncommon cause of ocular injury. The power of lightning is 10,000 to
2,00,000 amperes and a voltage of 20 million to 1 billion volts. Lightning
exposure time is only 1 to 100 milliseconds, taking less time to cause damage
of tissue5. Tissue destruction is caused by both thermal effect and
electrolysis. Non-nervous tissue offering high resistance is responsible for
the thermal effects of lightning resulting in rapid coagulation of the cellular
proteins. Lightning induced cataract is mostly bilateral. Possibility of
cataract formation increases with the proximity of the contact area to the eye6,7.
Lightning may reach its victims by any of the four routes and
causes injuries4,7:
1. Direct
strike: when the major current flows directly through the victim and is
facilitated by metal objects.
2. Splash:
where lightning strikes an object first and then arcs through the path of least
resistance.
3. Contact:
the bolt strikes an object the victim is in contact with i.e. electrocution
while telephonic conversation.
4. Ground
current: here the lightning travels along the surface towards the victim after
striking the ground.
Our
patient probably sustained the injury by the second mechanism mentioned;
lightning passed through the nearby coconut tree and through the ground.
Current passed initially through the left side of the body as indicated by left
sided hearing loss, poorer vision in LE (6/60) than RE (6/24) and denser
posterior sub-capsular cataract in LE. Severity of uveitis and macular damage
was also more in the LE.
In case
of bilateral cataract, it starts in the eye on the more affected side first and
there may be a gap of 1 – 10 months between the two eyes. Lightning induced
cataract may be attributed to, decreased permeability of lens capsule, protein
coagulation by electrical current, nutritional impairment of lens due to iritis
and mechanical damage to the lens fibers. Lightning induced cataract is
morphologically characteristic, affecting both anterior and posterior parts of
the lens. Regression of the opacity as a whole or partially has been reported7-11.
In our case there was both anterior and posterior-sub-capsular cataract in BE
(LE > RE).
The
macula is very sensitive to thermal damage because of the high melanin content
of the retinal pigment epithelium (RPE)3–4. Electrical
current damages the RPE by electrolysis. Melanin resists the electric current
leading to thermal denaturation of the outer retina and RPE. Lightning strike
may cause localized inflammation of the RPE. Retinal edema may result from
decreased transport of fluid out of retina or development of retinal vascular
incompetence3.
Early development of macular edema seen after lightning
strike may lead to formation of macular cyst, macular hole or solar maculopathy3,4. Lightning
maculopathy is supported by the lack of posterior vitreous detachment and
operculum3.
We
advised our patient macular hole surgery when she presented to us after the
injury but the patient denied. Subsequently after cataract surgery patient had
good visual outcome in both eyes. We presume that the hole had resolved on its
own which was clinically proven by negative Watzke – Allen sign (LE). Lightning induced macular
holes may undergo spontaneous closure with a good visual outcome4 which was a
feature in our case though there is no OCT documentation.
It is
important to differentiate between lightning induced macular cyst and
full-thickness macular hole, as cystic changes may resolve spontaneously but
for full – thickness macular whole surgery may be required12.
To the best of our knowledge, this is the first case
reporting bilateral lightning induced anterior and posterior segment ocular
damage with a good final visual outcome in both the eyes.
Author’s
Affiliation
Dr. Chandana Chakraborti
Assistant Professor
Dept. of Ophthalmology
Calcutta National Medical College and
Hospital
Kolkata 700006
West Bengal
India
REFERENCES
1.
Anastassios C. Koumbourlis. Electrical injuries. Crit Care Med. 2002; 30: 424-30.
2.
Norman ME, Albertson D,
Younge BR. Ophthalmic mani-estations of lightning strike. Surv Ophthalmol. 2001; 46: 19-24.
3.
Handa JT, Jaffe GJ. Lightning maculopathy. Retina. 1994; 14: 164-72.
4.
Lee MS, Gunton KB,
Fischer DH, Brucker AJ. Ocular mani-festations of remote lightning strike. Retina. 2002; 22: 808-10.
5.
David RL. Lightning
Induced Maculopathy. AECS
Illumination. 2012; 3: 20-22.
6.
Dimick AR. Harrison's Principles of
Internal Medicine. In: Fauci AS, Braunwald E, Isselbacher KJ, Wilson JD, Martin
JB, Kasper DL, et al., editors. Health Professions Division. 14th Ed. New York: McGraw-Hill.
1998: 2559.
7.
Rao KA, RAOLG, Kamath AN, Jain V. Bilateral macular hole secondary to
remote lightning strike. Indian J
Ophthalmol. 2009; 57: 470-2.
8.
Duke-Elder Sir S,
Macfaul PA. In: System
of Ophthalmology. Duke-Elder Sir S, editor. Vol XIV. London: Henry Kimpton. 1972; 2:
813-35.
9.
Biro Z, Pamer Z. Electrical cataract and optic
neuropathy. Int Ophthalmol.
1994; 18: 43-7.
10.
Hanna C, Fraunfelder FT. Electric cataracts I.
Sequential changes, Unusual and Prognostic Findings. II. Ultrastructural lens
changes. Arch. Ophthalmol.
1972; 87: 184.
11.
Wallace JF. Harrison's Principles of
Internal Medicine. In: Braunwald E,
Isselbacher KJ, Petersdorf RG, Wilson JD, Martin JB, Fauci AS, editors. Health Professions Division. 11th Ed. New York: McGraw-Hill.
1987; 859-60.
12. Moon SJ, Kim JE, Han DP. Photo Essay on lightning
induced maculopathy. Retina. 2005;
25: 380–2.