Original Article
Congenital
Cataracts; Its Laterality and Association with Consanguinity
Afia Matloob Rana,
Ali Raza, Waseem Akhter
Pak J Ophthalmol 2014, Vol. 30
No. 4
. . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
.. . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . .
|
See end of article for authors affiliations …..……………………….. Correspondence to: Afia Matloob Rana
Ophthalmology Department Holy Family Hospital, Rawalpindi Satellite Town, Rawalpindi Email: afiamatloob@yahoo.com …..……………………….. |
Purpose:
To study the frequency of laterality (bilateral vs. unilateral) and its
importance among congenital cataracts. We also investigated
consanguinity as a risk factor in congenital cataract cases. Material
and Methods: This study was
conducted in Ophthalmology department, Holy
family hospital, Rawalpindi, from 2nd January 2013 to 2nd
February 2014. A total of 112 eyes
and 86 patients in age range from 3 months to 26 years and all types of
visually significant congenital cataracts total or partial without prior history
of ocular trauma and syndromic association were recruited for the study.
Frequency distribution, test of significance was carried out using
Statistical Package for Social Sciences Version 20.0. Results: A total of 112 cases (61 males, 51 females) were recruited in the study. There was no statistically significant difference between different age groups and gender (p=0.2). The unilateral cases were 19.6% and bilateral were 80.4%. Consanguinity was present in 69.6% (n=78) and absent in 30.4% (n=34). The difference was statistically significant (p=0.00). Conclusion:
Bilateral congenital cataract is a more common
presentation as compared to unilateral cataract. Consanguinity is an
important risk factor for congenital cataract especially bilateral cataracts. Key Words: Congenital Cataracts; ocular trauma, Syndromic association |
Congenital cataract is an
important cause of preventable visual deprivation in children accounting for
5%-20% of blindness in children worldwide.1,2 World – wide, the
number of children who are blind is estimated to be 1.4 million, 190,000 of
them from cataract.3 Cataract in children can be classified as
congenital, developmental or traumatic.4
Congenital cataract presents
either from birth or shortly thereafter, while developmental cataract usually
refers to cataract that appears after the age of two5. Pediatric
cataracts are responsible for more than 1 million childhood blindness in Asia.6
The prevalence of cataract in children has been estimated about 3 in 10,000
live births.7 Ocular morbidity is mainly caused by obstruction to
development of the visual system and it has great physical, social economical
and psychological impact.
Prevention of visual
impairment and blindness in childhood due to congenital and infantile cataract
is an important international goal4 and is a priority for vision
2020.8 Epidemiology of congenital cataract is not fully understood
because it’s not a specific entity but combination of multiple factors,
including many associated ocular pathologies.
Density and laterality of
congenital cataract are one of the most important parameters in terms of visual
outcome, others are type of cataract, associated
ocular pathology and delay in presentation to hospital. Unilateral dense
cataract is a definite indication for early cataract surgery (preferably within
days) which is followed by aggressive amblyopia treatment, even then the
results mostly remain poor.9 Unilateral cataracts are generally
sporadic, with no family history of cataract or systemic illness, and affected
infants have history of full-term and normal health.9
Genesis of congenital cataract
is still not explored well and very little is known because of modern techniques,
long term accurate data needed and lack of sensitive investigative procedures.
Genetic factors are important in the etiology of congenital cataract, up to
half of childhood cataracts are genetic in origin10. Nearly,
one-third of total congenital cataract cases are familial.11 These types of cases are mainly because of genetically
induced developmental alterations among the crystalline lens and surrounding
tissues. There are a lot of ongoing epidemiological studies to find out risk
factors like intrauterine infections, certain enzymes deficiency, and sporadic.
The knowledge about the causes is important to develop appropriate planning
strategies, which are not available for many regions of the world and where
these are available, has been obtained mostly from studies of selected
populations, or from routine sources which are often based on small numbers of
cases.12
Routine ocular examination of young infants is
widely recommended to ensure that treatment, genetic counseling, and other
advice and support are offered at the earliest opportunity. The parents and any
siblings should be examined thoroughly even in the absence of positive family
history. In this study we are trying to analyse
frequency of laterality among congenital cataract and to investigate
consanguinity as risk factor among hospital data of congenital cataract in
patients attending our ophthalmology department.
MATERIAL AND METHODS
Our study includes patients
with congenital / infantile cataract presenting to Ophthalmology department, Holy
family hospital, newly diagnosed during the 12-month period from 2nd
January 2013 to 2nd February 2014 identified prospectively. It
include 112 eyes and 86 patients in age ranging from 3 months to 26 years and
including all types of visually significant cataracts total or partial without
prior history of ocular trauma and syndromic
association. All affected individuals underwent a detailed history and
ophthalmological examination. Morphological details of cataract including other
ocular associations and also detailed dilated fundus examination where possible
were recorded. Informed consent was obtained and detailed medical and family
history with especial emphasis on consanguinity was obtained by taking detailed
history from parents or guardian of children on admission using a standardized
questionnaire. Ophthalmic examination included assessment of the pupillary red
reflex with a direct ophthalmoscope, visual acuity or fixation and following
behavior checked according to age of patients, complete anterior segment
examination with slit lamp and retinoscopy was done, B-scan was also done where required. All patients
underwent irrigation and aspiration of cataract with or without IOL followed by
aphakic correction where required according to latest
recommendations. Laterality and association of consanguinity with congenital
cataract was noted and assessed.
Statistical analysis was performed using Statistical
Package for Social Sciences Version 20. Fisher exact test was performed to
determine statistically significant differences in the gender of the
population. A p value of <0.05 was taken to be significant in all analysis.
RESULTS
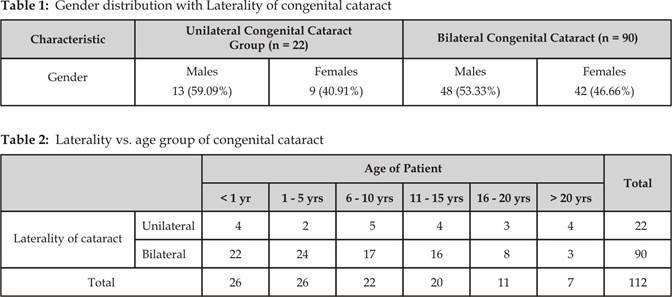
Congenital cataract characteristics and demographics of
the cases are shown in table 1 while table 2 shows laterality with age distribution,
picture 1 showing consanguinity with laterality while picture 2 showing
different morphological presentations of congenital cataract with gender
distribution.
A total of 112 cases (61 males, 51 females) were recruited
in the study. The distribution of congenital cataract cases for different age
groups in our study was as follows for less than 1 year age group 24.4% (n=15
males, n=11 females), age group 1–5 years 25% (n=19 males, n=7 females), age
group 6–10 years 19.6% (n=12 males, n=10 females), age group 11–15 years 17.9%
(n=8 males, n=12 females), age group 16–20 years 9.8% (n=4 males, n=7 females)
and age group more than 20 years 6.3% (n=3 males, n=4 females). There was no
statistically significant difference between different age groups and gender
(p=0.2). The bilateral cataracts (n=90) included 48 (53.33%) males
and 42 (46.66%) females, while unilateral cataract (n=22) comprised of 13
(59.09%) male and 9 (40.91%) female cases. In both bilateral and
unilateral cataract groups males were more as compare to females. This
difference was not statistically significant (p=0.093).
The cumulative unilateral cases were 19.6% and bilateral were 80.4%. In age
group less than 1 year 18% were unilateral and 24% were bilateral, in group 1-5
years unilateral were 9% and bilateral were 26%, in age group 6-10 years
unilateral was 23% and bilateral were 18%, in age group 11-15 years unilateral
were 18% and bilateral were 18%, in age group 16 – 20 years unilateral were 14%
and bilateral were 9%, in age group more than 20 years unilateral were 18% and
Fig. 1:
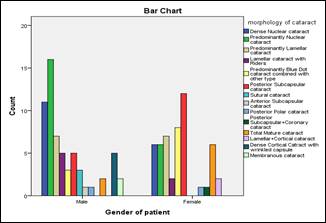
Fig.
2:
bilateral were 3%, there was no statistical significance (p=0.093) between age of presentation of congenital cataract
and laterality.
Consanguinity was present in 69.6% (n=78) and absent in
30.4% (n=34). The difference was statistically significant (p=0.00). Out of total cases with positive consanguinity 18%
(n=14) were unilateral and 82% (n=64) were bilateral while with absent
consanguinity 24% (n=8) were unilateral and 76% (n=26) were bilateral. There
was no statistically significant difference between the two groups (p=0.49).
In our study we also observed different morphologies of
cataracts. The frequencies of different types of congenital cataract were;
dense nuclear cataract 15.2% (n=11 males, n=6 females), predominantly nuclear
cataract 19.6% (n=16 males, n=6 females), predominantly lamellar cataract 12.5%
(n=7 males, n=7 females), lamellar cataract with riders 6.3% (n=5 males, n=2
females) f, predominantly blue dot cataract 9.8% (n=3 males, n=8 females),
posterior sub-capsular cataract 15.2% (n=5 males, n=12 females), sutural cataract 2.7% (n=3 males, n=0 females), anterior
sub-capsular cataract 0.9% (n=1 males, n=0 females), posterior polar 1.8% (n=1 males, n=1 females) , sub-capsular
coronary cataract 0.9% (n=0 males, n=1
females) , total mature cataract 7.1% (n=2 males,
n=6 females), cortical cataract 1.8% (n=0 males, n=2
females) , cortical cataract with wrinkle 4.5% (n=5
males, n=0 females), and membranous cataract 1.8% (n=2 males,
n=0 females). There was statistically significant difference between
gender and morphology of cataract (p =0.01).
DISCUSSION
Congenital cataract is a major cause of blindness in children. Congenital cataract is important in the regards that it blurs the retinal image as well as disrupts the development of the visual pathways in the central nervous system. Congenital cataract is a rare disease, but it is a major cause of low vision or blindness among both developed13 and developing14 countries. The causes for most of the congenital cataracts remained unknown.15,16 Prevention of visual impairment due to congenital and infantile cataract is an important component of world health organization’s international program for elimination of avoidable blindness by 202017. Surgical removal of the opacified lens with and without intraocular lens implantation is the only treatment available for congenital cataract.18
In our study male were 55%
(n=61) and females were 45% (n=51). Male to female ratio was similar to the
study of Mwende J et all19,
who had 55% (n=99) males and 45% (n=81). In the same study bilateral cataracts
were 66% and unilateral were 34%, while in our study it was 80.4% and 19.6%
respectively. Rahi JS et all20.
In their study also the same ratio of laterality 66% and 34% was observed
respectively. The difference was not statistically significant in both studies.
The difference between our study and the two groups was because of the included
age group which was more in our study from 3 month to 26 years while in the
rest of the two studies it was 1 year of age. Ruddle
JB et al,21 also observed in their study
that there was no significant difference between laterality of cataract
(bilateral 45.5% vs. unilateral 55.5%) or gender (p = 0.068). Laterality is one of
the most important parameters in terms of management. Unilateral cataracts have
poor prognosis as there are much more chances of amblyopia as compare to
bilateral. In unilateral congenital cataract prognosis for visual outcome after
cataract surgery depends on early clearance of visual axis, aphakic
correction, and aggressive amblyopia treatment. Congenital cataracts ideally
should be operated before three months of age.19
In our study cases presented
before one year of age group was 24.4% including 18% unilateral and 24%
bilateral. After one year of age 75.6% cases presented including 82% unilateral
and 76% bilateral. As we observed in our study that small number of cases
presented before one year of age and unilateral cataracts were less in numbers.
The reason was the early appreciation of reduced vision in bilateral cases.
Management of congenital cataract depends on the etiology, degree of visual
interference and laterality of cataract. The outcome of cataract surgery after
congenital cataract is 20 times worse than developmental cataracts, especially
for those cases which are operated after one year of age.22 The
visual system can get the opportunity to develop and mature after surgery while
its progress remains halted by the development of cataract and visual system
cannot develop at all in presence of dense congenital cataract 23.
That’s why early cataract surgery is important in congenital cataract.
Especially for severe bilateral cataracts which are causing significant
obscuration of the visual axis, surgery is recommended as early as possible.
In developing countries delay
in presentation and inadequate use of surgical services are the major causes of
blindness secondary to congenital cataract24. The visual outcome depends
upon the duration between onset of visual impairment and surgery, the shorter
the duration, higher likelihood of good visual outcome. Early presentation is
important for visual outcome, regardless the type of cataract. The reasons of
excessive delay of presentation in our study population were few barriers to
presentation, which include lack of awareness about the disease, difficult
access to health services, or acceptance of services (lack of education).
In the language of clinical
genetics, a consanguineous marriage is defined as a union between two
individuals who are related to each other as second cousins or closer, with the
inbreeding coefficient (F) equal or higher than 0.0156, where (F) is a measure
of proportion of loci at which the offspring is expected to inherit identical
gene copies from both partners. Among Arabs and south Indian communities the
inbreeding coefficient (F) is highest where it reaches up to 0.125.25
In our study we observed
statistically significant high rate of positive history of first cousin
marriage and among the positive cases bilateral cataracts were more common as
compare to unilateral cataracts. This high rate of observed consanguinity may
be considered as one of the risk factor for congenital cataract. At the same time
this aspect could not be overlooked that consanguinity is very common in
Pakistani families and this relationship of consanguinity with congenital
cataract as risk factor may be an incidental finding as number of our patients
were limited.
A significant positive
association has been consistently demonstrated between consanguinity and
morbidity, although consanguinity associated blindness is less frequent but an
increased rate of congenital cataracts has been reported in several
populations.26 One billion people are currently living in those
countries where consanguineous marriages are customary, and among them, one in
every three marriages is cousin marriage, with a deeply rooted social trend.
Public awareness is rising about preventive measures of congenital disorders
which has led to a trend that the number of couples who are seeking for
preconception and premarital counseling on consanguinity are increasing
gradually.27
The morphology of congenital
cataracts is also very helpful in establishing their etiology and prognosis.
Congenital cataract is inherited in all three Mendelian
forms: autosomal dominant, autosomal recessive, and X-linked. In view of
association of congenital cataract with consanguinity in literature, and the
need to identify and delineate the variability in congenital cataract, the
present study was undertaken to ascertain the role of consanguinity in
congenital cataract patients.
The prospective study of laterality and
consanguinity in congenital cataract has several limitations. Although we
believe that all patients included in our study had congenital cataract not all
patients were seen from time of birth .These cataracts showed many different
patterns. The underlying and associated factors in patients with congenital
cataract in this study were diverse. This complex pattern including variable
differences between unilateral and bilateral cataracts has implication for
further etiological research.
CONCLUSION
Bilateral congenital cataract is a more common presentation
as compare to unilateral congenital cataract..
Consanguinity is an important risk factor for congenital cataract especially
for bilateral cataracts.
Author’s Affiliation
Dr. Afia
Matloob Rana
Post Graduate Resident
Ophthalmology Department
Holy Family Hospital
Rawalpindi
Dr. Ali Raza
Associate Professor
Ophthalmology Department
Holy Family Hospital
Rawalpindi
Dr. Waseem
Akhter
Assistant Professor
Ophthalmology Department
Rawal Institute of Health Sciences
Islamabad
REFERENCES
1.
Halilbasic M, Zvornicanin J, Jusufovic V, Cabric E, Halilbasic A, Musanovic Z, Mededovic A. Pediatric cataract in Tuzla Canton, Bosnia and
Herzegovina. Med Glas (Zenica)
2014; 11:127-31.
2.
Santhiya ST, Kumar GS, Sudhakar
P, Gupta N, Klopp N, Illig
T, Söker T, Groth M, Platzer M, Gopinath PM, Graw J. Molecular analysis of cataract families in India: new mutations
in the CRYBB2 and GJA3 genes and rare polymorphisms. Mol Vis. 2010; 16:
1837-47.
3.
Randrianotahina HC, Nkumbe HE. Pediatric cataract surgery in Madagascar. Niger J Clin Pract. 2014; 17:14-7.
4.
Nkumbe HE, Randrianotahina HC. Meeting the need for
childhood cataract surgical services in Madagascar. Afr
J Paediatr Surg. 2011; 8:182-4.
5.
Bronsard A, Geneau R, Shirima S, Courtright P, Mwende J. Why are children brought late for cataract surgery? Qualitative
findings from Tanzania. Ophthalmic Epidemiol. 2008;
15: 383-8.
6.
World Health Organisation. Prevention of
childhood blindness. Geneva: WHO; 1992.
7.
Sana N, Muhammad A, Humaira F. Congenital Cataract:
Morphology and Management Pak J Ophthalmol. 2013; 29:
151-55.
8.
Global Initiative for the Elimination of Avoidable Blindness:
Action Plan. 2006-2011. 2007.
9.
Tuli SY, Giordano BP, Kelly M, Fillipps
D, Tuli SS. Newborn with an Absent Red Reflex. J Pediatr Health Care. 2013; 27: 51–5.
10.
Haiba KS. Amer R, Mariam S, Samra K, Nadeem HB, Ahmed UZ. Autosomal recessive
congenital cataract linked to EPHA2 in a consanguineous Pakistani family. Mol
Vis. 2010; 16: 511-17.
11.
Jochen G. Congenital hereditary cataracts, Int. J. Dev. Biol. 2004; 48:
1031-44.
12.
Jugnoo SR, Carol D. The British Congenital Cataract Interest Group
Congenital and Infantile Cataract in the United Kingdom: Underlying or
Associated Factors Invest. Ophthalmol. Vis. Sci.
2000; 41: 2108-14.
13.
Rosenberg T. Yearly Memorandum from the Danish National Register of the
Visually Impaired. 2002; 1–4.
14.
Ezegwui IR, Umeh RE, Ezepue UF. Causes of childhood blindness: results from schools for the blind
in south eastern Nigeria. Br J Ophthalmol. 2003; 87:
20–3.
15.
Bhatti TR, Dott M, Yoon PW,
Moore CA, Gambrell D, Rasmussen SA. Descriptive epidemiology of
infantile cataracts in metropolitan Atlanta, GA, 1968–1998. Arch Pediatr Adolesc Med. 2003; 157:
341–7.
16.
Haargaard B, Wohlfahrt J, Fledelius H, Rosenberg T, Melbye
M. A nationwide Danish study of
1027 cases of congenital/infantile cataracts: etiological and clinical
classifications. Ophthalmology. 2004; 111: 2292–8.
17.
Courtright P, Hutchinson AK, Lewallen
S. Visual impairment in children
in middle- and lower-income countries. Arch Dis Child. 2011; 96: 1129-34.
18.
Yorston D. Surgery for Congenital Cataract. Community eye health. 2004; 17:
23-5.
19.
Mwende J, Bronsard A, Mosha M, Bowman R, Geneau R, Courtright P. Delay in presentation to hospital for surgery for congenital and
developmental cataract in Tanzania. Br J Ophthalmol.
2005; 89: 1478–82.
20.
Rahi JS, Dezateux C. Congenital and Infantile
Cataract in the United Kingdom: Underlying or Associated Factors. Invest. Ophthalmol. Vis. Sci. 2000; 41: 2108-14.
21.
Ruddle JB, Staffieri SE, Crowston JG, Sherwin JC, Mackey DA. Incidence and predictors of
glaucoma following surgery for congenital cataract in the first year of life in
Victoria, Australia. Clin Experiment Ophthalmol. 2013; 41: 653-61.
22.
Magnusson G, Abrahamsson M, Sjostrand J. Changes in visual acuity from 4 to 12 years of age in children
operated for bilateral congenital cataracts. Br J Ophthalmol.
2002; 86: 1385-9.
23.
Khanna RC, Foster A, Gogate PM. Visual outcomes of bilateral congenital and developmental cataracts
in young children in south India and causes of poor outcome. Indian J Ophthalmol. 2013; 61: 65-70.
24.
Waddel KM. Childhood blindness and low vision in Uganda. Eye. 1998; 12:
184–92.
25.
Hamamy H, Antonarakis SE, Cavalli-Sforza LL, Temtamy S, Romeo G, Kate LP. Consanguineous marriages, pearls and perils:
Geneva International Consanguinity Workshop report. Genet Med. 2011; 13:841-47.
26.
Bittles AH, Black ML. The impact of consanguinity on neonatal and infant
health. Early Hum Dev. 2010; 86:737-41.
27.
Hamamy H. Consanguineous marriages. J Community Genet. 2012; 3:185-92.