Presentation of eye diseases vary worldwide1,4. studies
had shown that certain eye diseases are common in certain age, gender, and
occupation.4-6 Some eye morbidities and visual abnormalities of
children could affect their learning abilities, personality and adjustment in
school, to avoid such problems prompt and proper eye care is needed.2,3
While some eye diseases are just the cause of ocular morbidities and are easily
treatable, others if cannot treated or prevented timely can invariably leads to
blindness7 therefore it is important to find out the pattern of eye
diseases. Early diagnosis is required in some eye diseases to prevent vision
loss and optimized visual outcome.8
The years of early development make the
child particularly vulnerable to visual disorders, especially if the normal
development of the eye is affected by the occurrence of disease. This has been
documented by various authors as it may have a devastating impact on the
child’s psychological and physical development and his ability to learn.9
Children with poor vision may be considered by their teachers to be poor
students and both teachers and parents may subsequently lower their
expectations of the child’s performance.9
The aim of this study was to find out the pattern of eye diseases
of anterior chamber and adnexa oculi in children of pediatric ophthalmology
department of Layton Rehmatullah Benevolent Trust
(LRBT), Korangi – Karachi. It is the Pakistan`s
largest non-governmental organization which provide free eye care services and
works to fight against blindness.10
MATERIAL AND METHODS
This was a hospital-based cross sectional survey
with descriptive methodological design. All children aged 0 – 15 years
attending outpatient department in LRBT hospital Karachi, having diseases of
anterior segment of eye and adnexa oculi were included in the study while those
presented with the diseases of posterior segment of eye were excluded.
Children were selected randomly in duration
of 2 weeks in the month of May 2013. Data of 250 children aged 0 – 15 years
were recorded who have diseases related to anterior segment of eye and adnexa
oculi after examining by consultant ophthalmologist. Children were placed into
three age groups i.e, less than 1 year, 1 to 6 years
and 7 to 15 years of age A pre designed Performa was filled for every patient
consisting the examination details which includes bio data, personal history,
presenting complains, aided and unaided visual acuity, refractive error and
signs of eye and adnexa, ocular alignment was also been recorded. This
information was retrieved by methods of examination such as visual acuity
testing by using Snellen test (for school going
children),and by preferential looking system (for
younger children), refraction (subjective, objective and cycloplegic),
slit lamp examination, and fundoscopy. After
examination patients were provided treatment accordingly and those who need
further evaluation were called for follow up.
The recorded data was analyzed on SPSS 16.0
and are presented as simple frequencies or cross-tabulations. A chi-squared
test was used to compare variables.
RESULTS
Data of 250 patients was recorded where
male proportion was found to be higher i.e, 52.8 %
(n=132) and female constitute 47.2% (n=118) (Table 1). The ratio of bilateral
disease was found to be more than unilateral as 68.4% cases show bilateral
involvement and 31.6% were presented with unilateral presentation. Among three
age groups 19.6% (n=49) patients were of age less than 1 year, 40.8% (n=102)
were of age 1–6 years and 39.6% (n=99) children were belong to 7 – 15 years of
age group (Table 2).
Around 15 diseases were diagnosed such as
refractive error, amblyopia, NLD blockage, blephritis,
ptosis, chalazion, stye,
VKC / allergic conjunctivitis, infective conjunctivitis (viral and bacterial),
corneal opacity, keratitis, congenital cataract, traumatic cataract,
convergence insufficiency, and squint in the patients of LRBT hospital.
The proportion of disease as shown in
(Table 3) was VKC – vernal keratoconjunctivitis i.e.
24.8% was the most common ocular morbidity found in children of LRBT hospital
with male pre-dominance i.e., 16.0% and in female it was found to be 8.8%
followed by squint both convergent and divergent 15.2%, refractive error 14.8%
where astigmatism was common, mostly associated with diseases like squint, NLD
Blockage 14.0% which was common among the children of age less than 1 year,
congenital cataract 6%, amblyopia 4.4%, infective conjunctivitis including
viral and bacterial conjunctivitis was 4.4%, blepharitis
4.0%, ptosis 2.4%, traumatic cataract 2.0%, causes involve injury by needle,
chisel and edges of paper, followed by chalazion
1.6%, corneal opacity 1.6% and convergence insufficiency, keratitis and stye each constitute 0.4%.
A total of 37 children (out of 250) were
presented with refractive error, in which 15 (40.54%) patients were astigmatic,
7 (18.91%) were hypermetropic while 15 patients
(40.54%) were presented with myopia (Table 4).
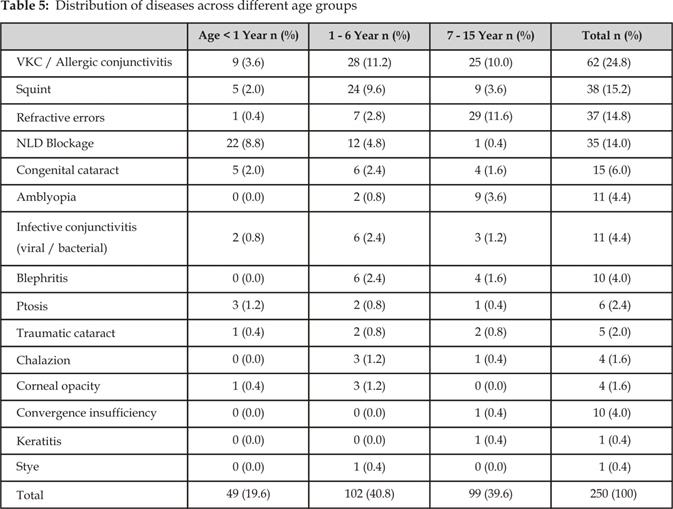
As 250 patients from age 0-15 are divided into three groups, the
second age group i.e. 1 – 6 years was presented with highest proportion of
diseases (40.8%), while 7 – 15 years group accounts for 39.6% patients followed
by less than 1 year group which constitutes 19.6% (Table 5). The most common disease found in 1 – 6 years was
VKC (11.2%) followed by squint (9.6%) out of total 40.8% cases from this age
group while children from 7 – 16 years were presented with refractive errors
mostly (11.6%) out of 39.6% and 8.8% out of 19.6% in age group less than 1 year
were presented with NLD blockage.
DISCUSSION
The major ocular disorder encountered in
our study was VKC – vernal keratoconjunctivitis which
was similar to the study of A.I Ajaiyeoba done in
South – Western Nigeria4 VKC is a chronic, bilateral inflammation of
the superior and limbal palpebral conjunctiva. The warmer the climate, the greater its prevalence. Onset
typically occurs between ages 3 and 25 years. Males typically are affected more
than females,11 although vernal or allergic conjunctivitis is not
usually a cause of blindness except with complications, it has been found to be
a leading cause of absenteeism from school and could compromise the quality of
life, impairing daily activities and work.8,13 males were found to
be more effected in our study and similar result was found in study conducted
by Zareen Mahdi at Sindh government hospital new Karachi12and
study done at Khyber Teaching Hospital Peshawar by Sadia
Sethi.15
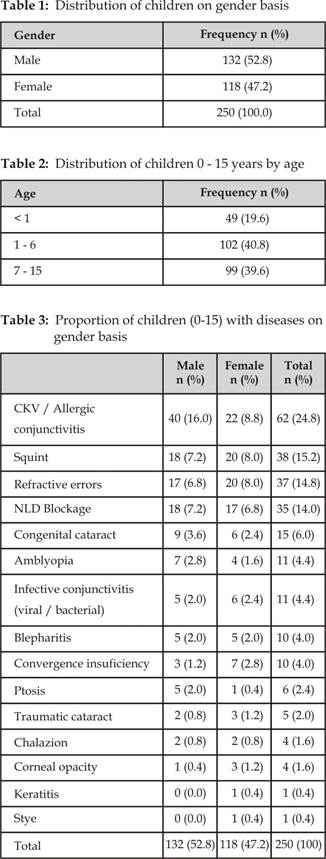
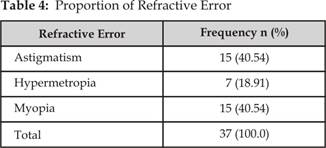
Fig. 1: Proportion of diseases on gender basis
Fig. 2: Proportion of
refractive errors
Total cases of squint registered were 15.2%
which was somehow similar with the study done in Sindh government hospital new
Karachi12. The ability of the eyes and the brain to work together
develops through-out childhood up to the age of about 8 years but particularly
within the first two years of life. If a child develops a squint, the eyes stop
working together and they stop developing the ability to work together
correctly which may lead to amblyopia a lazy eye.14
Refractive
error accounts for 14.8% majority of those belongs third age group (7 – 15
years) with same result as the study of Nigeria where refractive error account
for 14.3%,17 while in the study in Peshawar
the frequency of refractive error was 12.8%.15
In this study 8.0% children were having cataract in which the
ratio of congenital cataract was higher i.e. 6.0% whereas traumatic cataract
accounts for only 2%. The similar result were found in the study of Nigeria
where 6.6% children came with cataract17 cataract is the most common
cause of visual impairment in Pakistan followed by refractive error, retinal
diseases, glaucoma and conjunctivitis, if timely and appropriate treatment is
not initiated at the first sign of emerging eye problem these diseases can
cause blindness16.
The
ratio of NLD blockage in this study was found quite high i.e. 14.0% as compared
to the study at Khyber teaching hospital where NLD was found 5.4%15 and
at Sindh Government Hospital it was found 3.5%.12 The major affected
group (8.8%) was less than one year of age.
Eye
injuries remain a major cause of unilateral visual impairment worldwide18and
a common cause of non-congenital unilateral blindness.19Children are
particularly at risk of ocular injury due to their decreased ability to detect
and avoid potential hazards.18,21 Most childhood eye injuries are
sustained during unsupervised play and domestic activities.22-25 In
the study at South– Western Nigeria ocular trauma was the most common ocular
morbidity in children where 21.7% patients were presented with trauma17 and
in another study at Sindh Govt. trauma accounts for 9.6% cases12while
in this study very few cases i.e: 2.0% were reported,
usually presented with traumatic cataract and corneal opacity (1.6%).
Amblyopia
– lazy eye is the reason for permanent vision loss if not treated timely26
in this study amblyopia cases were found around 4.4% where as in the study at
South Karachi only 0.5% cases were reported27and in another study at
south western Nigeria 0.08% cases were found.28
Convergence
insufficiency is the leading cause of eye starin,
blurred vision, double vision and headache29 in this study 10 (4.0%)
children were presented with convergence insufficiency. They had complained of
headache with normal visual acuity 6/6.
Around 6 patients were presented with
ptosis, 4 with chalazion and 1 with stye, these external eye conditions are not threat to
vision. Ranking of these diseases were lowest in other studies30,31which
is similar to this study.
Eye infections are preventable but challenging cause of blindness,
in this study 11 patients were presented with infective conjunctivitis
including bacterial and viral conjunctivitis and only 1 patient had keratitis.
CONCLUSION
Male preponderance was more than females. The most common eye
disease found out in this study was vernal catarrh requires long term medical
treatment. Further Studies are required to find out the risk factors which
aggravate the symptoms and to find the etiology so that the incidence can be
minimized.
Author’s Affiliation
Bilqis Khatri
Research Assistant
&Ophthalmic Technologist.
Hashmanis Hospital
JM-75, Jacob lines, off M.A Jinnah Road, Karachi.
Ayesha Kashif
Ophthalmic Technologist
Graduated from DUHS
JM-75, Jacob lines, off M.A Jinnah Road, Karachi
REFERENCES
1.
Topalovo AV. Incidence of Eye Diseases in different parts of
the World. Ophthalmol. 1984; 6: 374-7.
2.
Pratab VB, Lai HB. Pattern of pediatric ocular problem in North India. India J Ophthalmol. 1989; 37: 171–2.
3.
Adegbehingbe BO, Adeoye AO, Onakpoya
OH. Refractive errors in
childhood. Nigerian Journal of Surgical Sciences. 2005; 15: 19–25.
4.
Ajayeoba AI, Scott SCO. Risk factors associated with
eye disease in Ibadan, Nigeria. Afr J Biomed Res.
2002; 5: 1-3.
5.
Canavan YM, O'Flaherty MJ, Archer DB. A Ten
-year Survey of Eye – Injuries in Northern Ireland. Br J Ophthalmol.
1980; 64: 618-25.
6.
Alakija W. Eye morbidity among welders in Benin City,
Nigeria. Public Health. 1988; 102: 381-4.
7.
Onwasigwe EN, Umeh RE, Onwasigwe
CN, et al. Referral pattern of children to the eye department of the
University of Nigeria Teaching Hospital, Enugu, Nigeria. Nigerian Journal of
Ophthalmology. 1996; 1: 5-6.
8.
Simon JW, Kaw P. Albany Medical College,
Albany, New York Am Fam Physician, 2001; 64: 623-9.
9.
Newcomb, D. Robert. Public health and
community optometry.2nd ed. Missouri, U.S.A.: Butterworth-Heinemann,: Saint Louis, 1990.
10.
LRBT[homepage on
internet]:available at::www.lrbt.org.pk
11.
Sowka JW, Gurwood AS, Kabat
AG. “Vernal kerato
conjunctivitis.” The Handbook of Ocular Disease Management. N.p.: JOBSON, 2001.
12.
Mahdi Z, Munami S, Sheikh ZA, Awan H, Wahab S. Pattern of eye diseases in children at secondary level eye
department in Karachi, Pak J Ophthalmol. 2006;
22:146-51.
13.
Joss JD, Craig TJ. Seasonal allergic
conjunctivitis: overview and treatment update. J Am Osteopath Assoc. 1999;
99:513–8.
14.
Squint
in Childhood." Royal National Institute of Blind People [home page
on inernet]. London N.p.,
n.d. available from:
http://www.rnib.org.uk/eyehealth/eyeconditions/eyeconditionsoz/Pages/squint.
aspx
15.
Sethi S, Sethi MJ, Saeed N, NK Kundi.
Pattern of common eye
diseases in children attending outpatient eye department Khyber Teaching
Hospital Peshawar, Pak J Ophthalmol. 2008; 24:
166-70.
16.
Mursalin S.M, Younus A, Iqbal
N, Rehman B, Malik IM. An
assessment of burden of eye diseases and surgeries in Pakistan, College of
ophthalmology and allied vision science. Accessed on 01-01-2014.
17.
Onakpoya OH. Childhood eye diseases in south-western Nigeria, Clinics. 2009;
64: 947.
18. Niiranem M, Ratvio
I. Eye
injuries in children. Br J Ophthalmol. 1981; 65: 436–8.
19.
Causes
of Childhood Blindness and Current Control Measures. "Prevention of
Childhood Blindness. Geneva: World Health Organization, 1992. pp. 21–22.
20.
Alhaski M, Almaaita J. Retrospective analysis of pediatric ocular trauma at Prince Ali
Hospital. Middle
East Journal of Family Medicine, 2007; 5: 42–5.
21. Olurin O. Eye injuries in Nigeria. A review of 433 cases. Am J Ophthalmol. 1971; 72: 159–66.
22.
Nwosu SNN. Domestic ocular and adnexa injuries in Nigeria. W Afr J Med. 1995; 14: 137–40.
23.
Kwari F, AlHassan MB, Abiose A. Pattern and outcome of peadiatric
ocular trauma – A 3 – year review National Eye Centre Kaduna. Nigerian Journal of Ophthalmology, 2000; 8: 11–6.
24.
Nkanga DG, Doln P. School vision screening in Enugu, Nigeria: Assessment of referral
criteria for refractive error. Nigerian Journal of Ophthalmology, 1997; 5: 34–40.
25. Adeoye AO. Eye injuries in the young in Ile Ife, Nigeria. Nig J Med. 2002; 11: 26–8.
26.
American Association for Pediatric Ophthalmology and Strabismus, [home page on the internet], accessed on 01-02-2014, available from: http://www.aapos.org/
27. Sheikh
SP, Aziz
TM.
Pattern of eye diseases in children of 5-15 years at Bazzertaline
Area (South Karachi) Pakistan, J Coll
Physicians Surg Pak. 2005; 15: 291-4.
28.
Ayotunde I. Ajaiyeoba, Pattern of eye diseases and visual impairment
among students in southwestern Nigeria, Int Ophthalmol. 2007; 27: 287–92.
29.
Cooper J, Cooper R. Conditions Associated with
Strabismus: Convergence Insufficiency. Optometrists Network, All About
Strabismus, 2001 – 2005.
30.
Abiose A, Allanson DB. Ocular health status of
post primary school children in Kaduna, Nigeria. Report of a survey. J Paediatr Ophthalmol Strab. 1980; 17: 337-40.
31.
Akinsola FB, Ajaiyeoba AI. Causes of low vision and
blindness in a blind school in Lagos, Nigeria. W Afr
J Med. 2002; 2: 63– 5.