Original Article
Pre-Operative Diclofenac Sodium Eye
Drops Vs Intra-Operative Adrenaline Irrigation in Maintaining Mydriasis during Extracapsular
Cataract Extraction
Jehanzeb Khan, Imran Ahmad, Mubashir Rehman, Zeeshan Tahir
Pak J Ophthalmol
2014, Vol. 30 No. 4
. . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . .. . .. . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . .
|
See end of article for authors affiliations …..……………………….. Correspondence to: Jehanzeb Khan Medical Officer Lady Reading Hospital,
Peshawar …..……………………….. |
Purpose:
To compare the effectiveness of
pre-operative diclofenac sodium eye drops with per-operative
intraocular irrigation with adrenaline 1:1,000,000 (one in one million)
solution in maintaining mydriasis during cataract
surgery. Material
and Methods: It was a randomized
control trial and was conducted in the department of Ophthalmology, Khyber
Teaching Hospital Peshawar from September 2010 to March 2011. 210 patients
with senile mature cataracts were divided into two groups “A” and “B” with
105 patients in each group. Group “A” received pre-operative diclofenac eye drops for 24 hours and group “B” received
per-operative irrigation with 1:1,000,000 of adrenaline solution. In all
patients pupillary size was measured after cortical matter removal during extracapsular cataract extraction. Results:
The mean age of patients in
group “A” was 59.87 ± 6.54 SD years and in group “B” was 61.38 ± 6.30 SD. The mean pupillary size after
cortical matter removal in group “A” was 7.0667 mm ± 1.78 SD while that in group “B” was
8.3371mm ±
1.94SD. The difference between the two was statistically significant after
applying independent sample‘t’ test with p value of
<0.000. Conclusion:
Per-operative irrigation of
adrenaline 1:1,000,000 solution keeps better pupillary size as compared to
pre-operative diclofenac sodium for patients
undergoing extracapsular cataract extraction, Key Words: Adrenaline, Extra capsular Cataract
Extraction, Diclofenac sodium |
Cataract surgery is one of the most common surgical procedures in
patients over the age of 60 years.1 Over
the past decade operative technique in cataract surgery has improved and the
operation has become less traumatic to the eye.2
Pupillary constriction during cataract surgery is found to be the
major cause of iris damage, incomplete cortex removal, posterior capsular
rupture, vitreous loss, and even posterior lens matter dislocation.3,4 Cataract surgery can be performed more easily and
safely if mydriasis can be maintained until
intraocular lens implantation.5 Different drugs e.g. cyclopentolate, tropicamide and diclofenac sodium have been used pre-operatively to
maintain per-operative pupillary dilatation.6,7
Per-operative intraocular irrigation with adrenaline 1:1,000,000
solution has been found to be safe and effective in maintaining mydriasis during cataract surgery.6
Pre-operative diclofenac sodium eye drops have also
been used and have found effective in maintaining mydriasis
during cataract surgery.8
Purpose
of the study was to determine the outcome of per-operative intraocular irrigation
with adrenaline 1:1,000,000 solution is better than pre-operative diclofenac sodium eye drops in maintaining mydriasis during cataract surgery that help in prevention
of complication. It is also cost effective and compliance is better than diclofenac sodium eye drops. No local study with such a
sample size had been carried out on this topic and this will help in changing
the protocol used for maintaining mydriasis during
cataract surgery.
MATERIAL AND METHODS
This
was a randomized control trial and was conducted at the department of
Ophthalmology of Khyber Teaching Hospital, Peshawar from September 2010 to
March 2011. All patients with age related cataracts that undergone extracapsular cataract extractions by the same surgeon were
enrolled in the study. Patients with complicated cataracts including cataracts
with uveitis, pigment dispersion syndrome, pseudoexfoliation,
lens related glaucoma, traumatic cataracts and patients with cardiac diseases,
diabetes and hypertension were excluded from the study to avoid biased in the
study results. Patients were diagnosed with slit – lamp examination and ophthalmoloscopy. Written informed consent was taken from
all patients. Pupil in patients of both groups was dilated with topical Tropicamide 1% eye drops (1 drop every 10 minutes for 45
minutes- 1 hour before surgery). These patients were randomly allocated into
“A” (diclofenac group) and “B” (adrenaline group) by
lottery method. Adrenaline 1:1,000,000 solution was made by diluting one
adrenaline ampule 1:1000 in 1 liter (1000 ml) of ringer lactate. Patients in
group “A” had mydriasis with pre-operative diclofenac sodium for 24 hours before surgery and patients
in group “B” were irrigated per-operatively with adrenaline 1:1,000,000
solution. Intra-operatively pupil size was measured with a caliper after
cortical lens matter removal during surgery. Exclusion criteria were followed
strictly to avoid any confounder and bias in study results. All the statistical
analysis was carried out using SPSS version 11.0. Student t-test was applied
between the pupil sizes of both the drugs to see their effects. P-value of ≤
0.05 was considered significant.
RESULTS
A total of 210 patients were enrolled in the study and were
randomly distributed in two groups A and B with 105 patients in each group. In
group A there were 71 (68.6%) male and 34 (32.4%) female patients, whereas in
group B there were 74 (70.5%) male and 31 (29.5%) female patients. All patients
enrolled have age range of 51 – 71 years with a mean of 59.87 ± 6.54
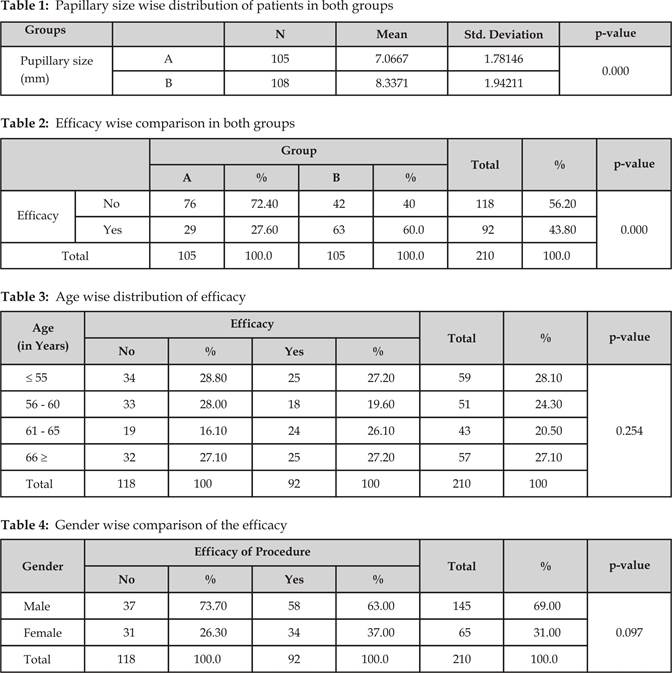
SD in group A and 61.38 ± 6.30 SD in group B. Average pupillary size in group A was 7.0667
mm ± 1.78 SD and in group B was 8.3371 mm ± 1.94 SD which was
highly significant with p-value = 0.000 (Table 1).
The efficacy of group A was 29 (27.6%) and group B was 63 (60%) (p-value = 0.000) (Table 2).
Age wise distribution of efficacy shows that 25 (27.2%) of
efficacy belongs to patients with age equal to or less than 55 years while 18
(19.6%) in age group of 56 – 60 years, 24 (26.1%) in 61 – 65 years while 25
(27.2%) efficacy was seen in above 66
years of age, which is significant with p-value = 0.254 (Table 3).
Efficacy
in male patients was 58 (63%) while in females it was observed in 34 (37%).
Majority of efficacy was shown in male as compared to female, although it was
not significant statistically with
p-value = 0.097 (Table 4).
DISCUSSION
Cataract extraction in majority of cases is a safe and effective procedure, but maintenance
of mydriasis can contribute to the ease with
which surgery can be performed.7 A small pupil during surgery
may increase the risk of damage to the iris, incomplete removal of soft
lens matter and more importantly, rupture of the posterior capsule
with vitreous loss.8 To maintain mydriasis
during surgery, various drugs have been used but it depends upon the surgeons
choice and available authentic literature9. The persistence of good mydriasis is a prerequisite for cataract surgery.10
Adequate use of preoperative mydriatics, subconjunctival mydricaine,
preservative-free intracameral adrenaline, iris
retractors and sphincterotomies are some of the
methods to combat poor mydriasis.11 Inspite
of all these measures, the problem of poor mydriasis
is still a problem for surgeons.12 Hence we undertook this study,
creating a new local data regarding the best mydriatic
among diclofenac sodium and adrenaline regimen to
enable us to achieve better mydriasis during cataract
surgery.
The
present study demonstrates that adrenaline 1:1,000,000 in the intraocular
infusion is of significant benefit in maintaining mydriasis during cataract surgery compared to diclofenac sodium. The mean age of patient in diclofenac sodium group was 59.87 ± 6.54 SD while that in
the adrenaline group was 61.38 ± 6.30 SD. The mean pupillary size at the time of cortical matter
removal in diclofenac sodium group was
7.0667 mm ± 1.78 SD while that in adrenaline group was 8.3371 mm ± 1.94
SD. The difference was statistically significant after applying
independent sample t-test with p-value of < 0.000. The results of our study
clearly verified that adrenaline 1:1000000 solution is quite effective in
maintaining mydriasis during cataract extraction
along with IOL insertion for age related senile cataract.
A study conducted by Flach AJ comparing
the pupillary sizes at various stages of extracapsular
cataract extraction. The average dilation in adrenaline group at 45minutes was
7.13 mm and that in diclofenac group was 5.88 mm.13
The difference achieved in both the dilating regimens
was 1.25 mm which was statistically significant using the unpaired t-test (p
< 0.001). The results of this study were quite comparable and in close
approximation to what are achieved in our study.
Similar
results were obtained in a study conducted by Ong-Ton
L, he concluded his results showing better efficacy of adrenaline over diclofenac sodium as mean pupil diameter after cortical
lens matter removal was 8.14 mm ± 0.85 for adrenaline and 7.87 mm ± 1.03 for diclofenac sodium and the difference was statistically
significant (p < 0.002).6 These results were quite closer to what
we found in ours study.
Fig. 1:
Ender wise comparison of efficacy
Fahimi MS et al also demonstrated
similar results in his study for pupillary size during ECCE with a p-value of
< 0.04 proving that the difference between in pupillary size is
statistically significant.13 And even a much stronger difference has
been quoted by Guadalupe Cervantes-Coste with the
mean pupil size at the end of surgery, between diclofenac
sodium (6.84 ± 0.93 mm) and adrenaline group (7.91 ± 0.74 mm) was statistically
significant (p < 0.001).14
Similarly in a study conducted by Bäckström G, showed that there was a greater degree of
contraction in the absence of adrenaline in the irrigation solution (2.3 ± 1.0 mm
in the intracameral mydriatics
(ICM) group and 3.2 ± 0.7 mm in the placebo group (p = 0.015).15
Our
study has shown that per-operative intraocular irrigation with adrenaline
1:1000,000 has significant benefit in maintaining mydriasis during cataract
surgery.
CONCLUSION
Per
operative irrigation of adrenaline 1:1,000,000 solution keeps better pupillary
size compared to pre-operative diclofenac sodium for
patient undergoing extracapsular cataract extraction.
Author’s Affiliation
Dr. Jehanzeb Khan
Medical Officer
Department of Ophthalmology
Lady Reading Hospital, Peshawar
Dr. Imran Ahmad
Medical Officer
Pakistan Institute of Community Ophthalmology
Hayatabad Medical Complex, Peshawar
Dr. Mubashir Rehman
Medical Officer
Lady Reading Hospital, Peshawar
Dr. Zeeshan Tahir
Medical Officer
Lady Reading Hospital, Peshawar
REFERENCES
1.
Reeves SW.
Advances in cataract surgery and intraocular lenses. Clinical and health
affairs. Ophthalmol. 2005; 103-19.
2.
Ocampo VVD,
Foster CS. Cataract, Senile:
Treatment and medication. E-medicine
specialties >ophthalmology>lens May 2009.
3.
Liou SW,
Yang CY. The effect of intracameral adrenaline infusion on pupil size, pulse rate,
and blood pressure during phacoemulsification. J Ophthalmol
and therapeutics. 2009; 14: 357-61.
4.
MS, Sheikh A, Fasih U. Comparative study of diclofenac sodium
with adrenaline for prevention on intra operative miosis.
Ann ABBASI Shaheed hosp
Karachi med dent coll. 2005 10: 729-31.
5.
Hirowatari T, Tojuda K, Kamei Y, Miyazaki Y, Matsubara M. Evaluation of a new preoperative ophthalmic solution. Can J Ophthalmol. 2005; 40: 58-62.
6.
Ong-Tone
L, Bell AJ. Cataract Refract Surg. Pupil size with and without adrenaline with diclofenac use before cataract surgery. 2009;
35:1396-400.
7.
Rafnsson V, Olafsdottir E, Hrafnkelsson J, Sasaki H,
Arnarsson A, Jonasson F. "Cosmic radiation increases the risk of nuclear cataract in
airline pilots: a population-based case-control study". Arch Ophthalmol. 2005; 123: 1102-5.
8.
Finger, Stanley. Origins of Neuroscience: A History of
Explorations in to Brain Function. Oxford University
Press. 1994; 70: 22-8.
9. Zigler Jr JS. Pathogenesis of cataracts. In: Tasman W, Jaeger EA, eds. Duane's Ophthalmology. 15th ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 2009.
10.
Howes FW. Indications for lens surgery/indications for application of
different lens surgery techniques. In: Yanoff M, Duker JS, eds. Ophthalmology. 3rd ed. St. Louis, Mo: Mosby
Elsevier; 2008.
11.
Hargrave SL,
Jung JC, Fini ME, Gelender
H, Cather C, Guidera A, et al. Possible role of vitamin E solubilizer
in topical Diclofenac on matrix metalloproteinase
expression in corneal melting: an analysis of postoperative keratolysis.
Ophthalmology. 2002; 109: 343-50.
12.
Corbett MC, Richards AB. Intraocular adrenaline maintains mydriasis
during cataract surgery. British Journal of Ophthalmology. 1994; 78: 95-8.
13.
Flach AJ. Corneal melts associated with topically applied nonsteroidal anti-inflammatory drugs. Trans Am Ophthalmol Soc.
14. Cervantes-Coste G, Sánchez-Castro YG, Orozco-Carroll
M, Mendoza-Schuster E, Velasco-Barona C. Inhibition of surgically induced miosis
and prevention of postoperative macular edema with diclofenac.
Clin Ophthalmol. 2009; 3: 219-26.
15. Bäckström G, Behndig A.
Redilatation with intracameral
mydriatics in phacoemulsification surgery. Acta Ophthalmol Scand. 2006; 84: 100-4.