The human retina and vitreous are bound
together by an intervening tissue called internal limiting membrane which acts
as a junction for the proliferation of various cells. Diseases of the macula
i.e. epimacular membranes and macular holes commonly involve the internal
limiting membrane. The constituents of internal limiting membrane include collagen, proteoglycans, basement membrane
and plasma membranes of muller cells and myofibrocytes. It is believed that
Contraction of these myofibrocytes leads to an enlargement of macular hole thus
preventing its closure. Therefore removal of internal limiting membrane from
the macula leads to closure of macular holes by inducing gliosis. As the
internal limiting membrane is a transparent structure so its removal is a very
delicate and difficult procedure as it may lead to inadvertent trauma to
retina. Difficult visualization of the internal limiting membrane and its firm
attachment to the underlying retina can present technical challenges while
trying to peel this membrane.1
The problem of visibility of internal
limiting membrane has been greatly reduced with the introduction of vital dyes
to stain the internal limiting membrane.
Trypan blue is one of the first dyes used to stain the
internal limiting membrane. It is successfully being used to stain the anterior
lens capsule in surgery of cataracts with absent red reflex.2 Now a day's trypan blue is widely being used in posterior
segment surgeries as epiretinal or internal limiting membrane peel and cystoids
macular oedema surgery. Up till now Trypan blue has not been shown
to be associated with any per operative complications such as staining of
retinal pigment epithelium cells leading to cell death as with indocyanin
green. Previously indocyanin green was being used in epiretinal membrane and
macular hole surgery. It was superior to trypan blue
in staining the internal limiting membrane but was toxic to retinal pigment
epithelium where trypan blue is superior in having no such adverse effects and
better visual and functional outcomes.3
Brilliant blue G also known as coomasian
blue has recently been reported as a tool in chromovitrectomy. It has been
widely used for protein staining in biological fields as it non-specifically
binds to most proteins. Brilliant blue G stains internal limiting membrane more
effectively than other dyes used for staining ILM, ERM and lens capsule. It is
easier to handle and is in granular form so that it is easily dissolved at a
stable Ph. Histological analysis shows that it has no toxic changes on retinal
layers and also successful peeling of ILM occurs without any remnant retinal
cells.4
Brilliant blue G is comparable to other dyes with
regard to visual and functional outcomes but is superior to then as it only and
selectively stains ILM. The purpose of this study is to compare ILM peel assisted
with trypan blue and brilliant blue G.
MATERIAL AND METHODS
This study was conducted at Mayo Hospital, Institute Of Ophthalmology, Eye Unit III, over duration of two years (1-3-12 to 28-2-14). 60 patients with stage 3 and 4 macular hole were included which were divided into two groups each containing equal number of patients. All patients with idiopathic macular holes were included while patients with rehgmatogenous retinal detachment and myopic / traumatic macular hole and those with ERM were excluded on slit lamp examination of the retina and OCT. Informed consent was taken from the patients followed by detailed history and complete examination of the anterior and posterior segments with the help of slit lamp bimicroscopy and indirect ophthalmoscope. Pre operative OCT was done to stage the macular hole. Post operative OCT was done at 1 week and 1 month to check for anatomical closure. Pre and post operative visual acuity was recorded to check for visual outcome. In the group A patients internal limiting membrane peeling was done with the assistance of brilliant blue G while group B patients underwent internal limiting membrane peeling with adjunctive trypan blue.
In group A patients, after induction of
posterior vitreous detachment, air was injected, brilliant blue G (0.5 ml, 0.25
mg/ml) was sprayed over the macular area followed by an air fluid exchange and
internal limiting membrane peeling after about one minute of spraying.
Similarly the group B patients underwent the same procedure but with the
assistance of trypan blue (0.5 ml, 0.06%). In all the patients SF6
was used after internal limiting membrane peeling and patients were advised face down posture for one week.
RESULTS
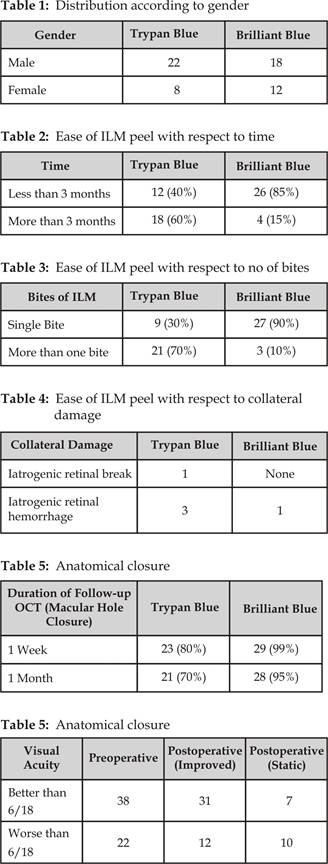
60 patients with ages between 40 to 60 years
were included in study over a period of one year. In group A there were 18 male and 12 female patients while group B comprised of 22 male and 8 female patients. In group A
internal limiting membrane peel was successfully done in 27 patients in first bite while 3 patients underwent the procedure in more
than two bites. In group B only9 patients underwent internal limiting
membrane peeling successfully in the first bite (p value 0.037) while 21 patients required more than one bite.
Internal limiting membrane peeling was completed within three minutes in 26 patients in group A as compared to 12 patients in group B (p value 0.002). There
was 1 iatrogenic break and 3 iatrogenic retinal hemorrhages in group B as
compared to only 1 iatrogenic hemorrhage in group A.
DISCUSSION
Vitreo retinal surgeons are commonly performing
peeling of internal limiting membrane now a days. Various macular disorders such as macular
hole, epiretinal membrane tractional macular oedema and vitreomacular traction
syndrome are being treated by doing peeling of internal limiting membrane.5
Indocyanin green was first introduced in ophthalmology
for the study of choroidal circulation. Later on it
was used in the posterior segment surgery to stain the transparent internal
limiting membrane during macular hole surgery.6
In macular hole surgery the concentration of indocyanin
green injected into the air or fluid filled vitreous cavity ranges from 0.25 to
0.50 mg/ml.7
Application of Indocyanin
green changes the light absorption properties of the ILM and increases the
stiffness of the membrane. The indocyanin green
potentiated light toxicity can be prevented by using a filter that could block
the wavelengths beyond 620 nm.8
Trypan blue is a vital stain which has been widely
used in ocular surgery. In ocular surgery a concentration of 0.06 to 0.15% is
used. Internal limiting membrane
staining with trypan blue is subtler than with indocyanin green probably
because trypan blue only stains a mild epiretinal membrane above the internal
limiting membrane rather than itself.9
The latest application of trypan blue in
chromovitrectomy is in the staining and localization of retinal breaks during
vitrectomy for retinal detach-ment. 0.15% trypan blue is injected
transretinally.
Gandorfer et al concluded in their research that trypanblue
staining promoted no ultra structural retinal damage but there were fragments
of muller cells adherent to retinal side of internal limiting membrane and
muller cell end feet were avulsed and ruptured.10
Naryanan et al also examined the effect of trypan blue
exposure on human RPE cells using the dye exclusion method and concluded that trypan blue at all
concentrations did not affect RPE cells with or without light exposure.
Brilliant blue G has emerged as a leading dye among all the
vital dyes in staining the internal limiting membrane during vitrectomy.
Brilliant blue G shows no retinal toxicity or adverse effects such as ganglion
cell death and retinal pigment cell atrophy which is seen with the use of other
dyes.
Recently modifications have been made in
Brilliant blue G by mixing it with 10% dextrose and heavy water thereby making
it dense than vitreous and intraocular fluids. This modification serves two purposes.
First the dye accumulates on the posterior pole rather than spreading in the
vitreous thus making the macular contact time prolonged. Secondly less amount
of dye is used both in terms of volume and concentration.11 Atul
Kumar12 et al compared brilliant blue G and triamcinolone acetonide
in internal limiting membrane peeling. It was concluded that there was a
statistically significant difference in the visual acuity of both the groups
making brilliant blue g with better visual outcome.
Machaida S13 et al compared the cone
electrore-tinograms after ICG, BBG and TA assisted macular hole
surgery. The a and b wave potentials were generally decreased in all the
patients but the photopic sensitivity response was significantly decreased in
patients undergoing surgery with the assistance of ICG as compared to normal
responses in patients treated with adjunctive BBG. Baba T14 et al compared vitrectomy
with brilliant blue G and indocyanin green and its effect on functioning of the
eye. The best corrected visual acuity was better in the brilliant blue G group.
The mean retinal sensitivity significantly improved in the BBG group. They
concluded that brilliant blue G was better in making the visibility of internal
limiting membrane as well as having minimal side effects. Doaa Awaad15
et al studied the toxic effects of brilliant blue G and trypan blue. In their
study the exposed the cultured human retinal pigment
epithelial cells to the trypan blue and brilliant blue g at varying
concentrations and time. They concluded in their study that trypan blue was
more toxic to the cultured human retinal epithelial cells at all concentrations
and times of exposure. Also brilliant blue g was more safe
in maintaining the integrity of Muller cells after internal limiting membrane
peeling for macular hole.
Shukla R16 et al compared trypan blue,
brilliant blue g and indocyanin green in their ease in internal limiting
membrane peeling.
The brilliant blue g group had a better post
operative visual acuity and less visual decline as compared to other groups.
Based on these observations it was concluded that BBG was comparable with
trypan blue in optimizing visual function while it was similar to ICG in ease
of internal limiting membrane peeling. But it was associated with less side effects
and toxicity as compared to other two groups.
In our study we compared brilliant blue g and
trypan blue in internal imiting membrane peeling with respect to staining,
timing of membrane eeling, number of bites of internal
limiting membrane during peeling and collateral damage (retinal break or
hemorrhage).
It was observed that 26
patients underwent membrane peel within three
minutes while 4 surgeries took more than five minutes
in brilliant blue G group. Similarly 12 patients underwent membrane peel within three
minutes and the rest took more than three
minutes in the trypan blue group.
27
surgeries were completed with first bite while 3 required more than one bite in the
brilliant blue g group. Similarly only9 membrane peel were done with first bite
while the rest 21 required more than one bite. There
was 1iatrogenic retinal break during surgery while 3 patients
had iatrogenic retinal hemorrhage in the trypan blue Group as compared to only
one iatrogenic retinal hemorrhage in the brilliant blue G group during surgery.
Follow up OCT was done to see the anatomical
closure. 29 macular holes in brilliant blue G group and 28 macular holes in the
trypan blue group were closed on OCT after one month of surgery.
Post operatively visual acuity improved in 43 patents out
of 60 while 17 patients showed no improvement or worsening in visual acuity.
CONCLUSION
Based on above observations in our studies we conclude that
brilliant blue G is more efficacious in staining the internal limiting membrane
leading to a statistically significant ease
in visibility, peeling, shorter surgery time and less side effects and
less collateral damage (though not statistically significant) but still
significant clinically as compared to trypan blue.
Author’s Affiliation
Dr. Chaudhary Nasir Ahmad
College of Ophthalmology and Allied Vision Sciences
(COAVS),
King Edward Medical University / Mayo Hospital,
Lahore
Dr. Muhammad Shaheer
College of Ophthalmology and Allied Vision Sciences
(COAVS),
King Edward Medical University / Mayo Hospital, Lahore
REFERENCES
1.
Kagimoto HTS, Hishatomi T, Eneida H,
Ishibashi T. This potent stain is easy to handle with minimal side
effects. Retina Today. 2001; 45-48.
2.
Gerrit RJM, Peter WTD, Jan HP, W
Houdijn B. Trypan blue staining to visualize capsulorhexis during
cataract surgery. Journal of cataract and refractive surgery. 1999; 25: 7-9.
3. Jeffery SG, Alain AP, John RG, Alexandar JM, Cindy MLH. Comparison of in vitro toxicity of indocyanin green to that of trypan blue in human retinal pigment epithelium cell cultures. American Journal of Ophthalmology. 2004; 138: 64-9.
4.
Nithani P, Vashisht N, Khunduja S, et al. Brilliant blue G assisted peeling of internal limiting membrane
in macular hole surgery. Indian J Ophthalmol. 2011;
59: 158-60.
5.
Abdelkader E, Louis N. Internal limiting membrane peeling in vitreoretinal surgery. Surv
Ophthalmol. 2008; 53: 368-96.
6.
Kadonosono K, Ito N, Uchio
E, Nakamura S, Ohno S. Staining of internal limiting membrane in
macular hole surgery. Arch Ophthalmol. 2000; 118; 1116-8.
7.
Ando F, Sasano K, Suzuki F. Indocyanin green assisted
ILM peeling in macular hole surgery revisited. Am J
Ophthalmol. 2004; 11: 2246-53.
8.
Wollensak G. Vital dyes in
vitreoretinal surgery. Dev Ophthalmol. 2008; 42: 82-90.
9.
Farah M, Maia M, Furlani B,
Bottos J, Meyer C, Lima V, Penha F, Costa E, Rodrigues E. Current concepts of trypan
blue in chromovitrectomy. Dev Ophthalmol. 2008; 42: 91-100.
10.
Gandorfer R, Rohleder M,
Charteris DG, Sethi C, Kempik A, Luthert P. Staining and peeling of
the internal limiting membrane in cat eye. Curr Eye Res 2005; 30: 977-88.
11.
Shukla D, Kelliath J,
Patwardhan A, Kannan NB, Thayyil SB. A preliminary study of
heavy brilliant blue G for internal limiting membrane staining in vitreoretinal
surgery. Indian Jr of Ophthalmology. 2012; 60: 531-4.
12.
Kumar A, Gogia V, Shah VM,
Sinha S. Brilliant blue G versus triamcinolone assisted ILM peeling: A
comparitive evaluation in macular hole surgery. World
journal of retina and vitreous. 2011; 1: 1-4.
13.
Machida S, Toba Y, Nishimura T, Ohzeki T, Murai K, Kurosaka D. Comparisons of cone electrograms after indocyanin green,
Brilliant blue G, or triamcinolone assisted macular hole surgery. Greafe arch
clin exp Ophthalmol. 2014; 252: 1423-33.
14.
Baba T, Hagiwara A, Sato E, Arai M, Oshitari T, Yamamoto S. Comparison of vitrectomy with indocyanin green or brilliant blue g
on retinal microvasculature and function of eyes in macular pathology.
Ophthalmology. 2012; 119: 2609-15.
15.
Awaad D, Schrader I, Bartok M, Mohr A, Gabel D. Comparitive toxicology of brilliant blue , trypan blue and their
combination together with polyethylene glycol on human pigment epithelial
cells. Investigative science and visual ophthalmology. 2011; 52: 4085-90.
16.
Shukla D, Kelliath J, Neelakantan N, Naresh K, Ramasamey K. A comparison of brilliant blue g, trypan blue and indocyanin green
dyes to assist internal limiting
membrane peeling during macular hole surgery. Retins. 2011; 31: 2021-5.