Pterygium is an abnormal fibrovascular
conjunctival tissue which encroaches the cornea.1
It is triangular in shape and is more frequently located nasally then
temporally.2 Ocular irritation, hyperemia and vision loss are the
most common clinical symptoms of pterygium.3 Early complaints e.g.
foreign body sensation and inflammation are treated conservatively with
artificial tears and anti-inflammatory drops to give symptomatic relief.4 However
surgical excision remains the main treatment for pterygium
causing visual impairment, cosmetic deformity, restriction of ocular motility
or marked irritation or discomfort unrelieved by medical management.5
Recurrence is the most common
postoperative complication after pterygium excision.5
In the past pterygium was treated surgically
with bare scleral technique.2 However this technique had a very high
recurrence rate of about 24 – 89%.2 Various techniques have been
applied in the recent years to reduce the recurrence rate which include pterygium resection combined with conjunctival
auto-graft, conjunctival resection with ammotic membrane graft and conjunctival
resection with stem cell transplantation.6 Surgical excision with conjunctival auto graft is not only safe and effective but
it also reduces the recurrence rate.7 Amniotic membrane
transplantation after surgical excision of pterygium
also appeared to be safe and effective with reduced rate of recurrence.8
Purpose of our study is to compare the efficacy of pterygium
resection combined with cojunctival auto graft versus
pterygium resection combined with amniotic membrane
graft in our population. Pterygium is a very common
ocular disease presenting to eye department. Main treatment modality in our set
up is surgical excision but majority of these patients presents again with
complaints of recurrence which is the most common post-operative complication.
It not only disturbs daily life of patient but also put economic restrain on
them. Also these patients put extra burden on OPD and OT. So in this study we
wanted to find out the surgical procedure which reduces the recurrence rate to
reduce burden on both patients and hospital.
MATERIAL AND METHODS
All patients were selected from eye OPD,
Lady Reading Hospital, Peshawar. Patients between the age of 20 to 50 years
both males and females, with primary pterygium of
size between 2 to 4 millimeter presenting within 6 months of onset were
included in the study. (In our set up pterigium
between 2 mm to 4 mm usually presents within 6 months of onset, long duration pterigium were excluded to avoid pterium
larger in size than 4 mm) Patients with recurrent pterygium,
pterygium associated with other chronic ocular
surface disease, patients on long term topical steriods
or topical NSAIDS, patients with previous history of any surgery on conjunctiva
and patients with pterygium of size less than 2 mm
and greater than 4 mm were excluded from the study. (pterigium of size 2 mm to 4 mm are more common so
included in the inclusion criteria so as to make sample collection easier).
Complete slit lamp examination was
performed for pterygium. The purpose and benefits of
the study was explained to all patients and if agreed upon a written informed
consent was obtained. The amniotic membrane was only taken from those patients
who have undergone cesarean section and properly screened out pre operatively.
Patients were divided into two groupsi.e Group A who underwent pterygium excision with conjunctival
autograft and Group B who were underwent pterygium excision with amniotic membrane graft.
Follow up was on 3rd month
postoperatively.(we have followed the patients every
three monthly, so follow up of first visit mentioned. On postoperative visit
patient was examined on slit lamp for recurrence of pterygium.
Surgery was considered effective with no recurrence of pterygium
and not effective with recurrence of at least 2 mm. The data was analyzed using
SPSS version 16.Frequencies and percentages were calculated for categorical
variables like gender, side of the eye and effectiveness. Mean and standard
deviation were calculated for numerical variables like age and duration. Chi
square test was used to compare the effectiveness of both groups. P value of
less than or equal to 0.05 was considered significant. Effectiveness in both
groups was stratified among age, side of the eye and gender to see the effect
of modifiers. All the results were presented as tables and charts. Post
stratification chi square test was applied.
DISCUSSION
Pterygium is one of the most common disorders in tropical
and subtropical region including Pakistan9. The most important risk
factors are exposure to sunlight, hot, windy dry weather and old age10.
Short body height is also cited in literature as a risk factor for
pterygiumdevelopment.11 (It has been mentioned in the literature for
which reference no 11 is given) It causes irritation, redness and affects the
visual acuity either by directly affecting the visual axis or by producing
changes in the corneal curvature.12 Prabhasawatetal9
conducted study on a total of 120 eyes in which 106 eyes had primary and
14 eyes had recurrent pterygia and showed that at 6
month after surgery conjunctival auto grafts
had a recurrence rate of 13.3%. In our study the recurrence rates in both
groups were higher than those reported previously, possibly because of amount
of subconjunctival tissue removal, race of our
population, type of suture used and drug given after surgery. Tananuvat N et al10 in their study showed the
recurrence rate of 12% in conjunctival auto graft
group and 22% in amniotic membrane graft group which is in accordance to our
study. Soloman A et al11
conducted study on 167 eyes, which included 148 primary and 19 recurrent pterygia. They showed that after 6 months the recurrence
rate in the amniotic membrane graft group was 28.1%. With the longer follow-up,
the recurrence rates were 25.0% and 12.3% for amniotic membrane graft and conjunctival graft respectively. Rahman
L et al13 had shown that conjunctival auto
grafts and amniotic membrane grafts differ in final appearance not only with
respect to the rate of recurrence but also in the percentage of normal
appearance. They suggested that covering the defect area with normal conjunctival tissue also has a higher likelihood of
promoting the restoration of a normal appearance. In a study conducted by SaleemM et al14 it was
shown that amniotic membrane contain a thick basement membrane and a vascular
matrix. The basement membrane reinforces adhesion of basal epithelial cells,
facilitates migration of epithelial cells, promotes epithelial differentiation
and prevents epithelial apoptosis. All these features promote rapid epithelialisation. Narsani AK et
al15 in their study showed that after pterygium
excision, amniotic membrane grafts are less effective than conjunctival
auto grafts in reducing recurrences. Even if there is a recurrence conjunctival auto graft should be considered as the first
choice for pterygium excision. However amniotic
membrane graft can also be considered as first choice in certain situations
e.g. those with advanced and diffuse conjunctival
involvement or when it is needed to preserve the bulbar conjunctiva for
glaucoma surgery. In similar study Katbaab A et al16 first compared amniotic membrane graft
(54) to a retrospective study using conjunctival auto
graft (122) in both primary and recurrent pterygium.
They noted that the recurrence rate is 10.9% using amniotic membrane graft,
which is still higher than 2.6% of conjunctival
graft. Nevertheless, both results of amniotic membrane grafts and conjunctival auto grafts are significantly better than the
primary closer, which resulted in 45% high recurrence rate for primary pterygium which is comparable to our study. Fallah MR et al17 showed in their study that by
removing larger amount of subconjunctival fibrosis
tissue and injecting long acting steroids, amniotic membrane grafts achieved a
recurrence rate of 3.0%, as compare to conjunctival
auto grafts with a recurrence rate of 2.6%. Similarly Lateefur-rehman
et al13 during follow up period, showed that recurrence of pterygia was high 41.33% in the patients with Bare sclera
method as compared to recurrence 33.33% while using 5-Fluorouracil antimetbolite. Ashok Kumar Narsani
et al15 showed that there was 7.69% recurrences in conjunctival auto graft as compared to 16.13% recurrences
with amniotic membrane graft.
RESULTS
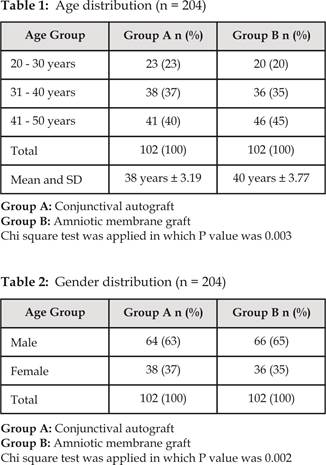
Age distribution among two groups is shown in Table 1. In group A mean age
was 38 years ±3.19, where as in group
B mean age was 38 years ±3.77.
Gender
distribution among two groups was analyzed as in group A 64(63%) patients were male and 38(37%) patients were female.
Where as in group B66(65%)
patients were male and 36(35%) patients were female in Table 2.
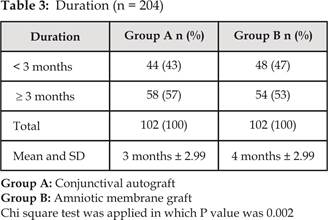
Duration of pterygium between two groups
was analysed as in group A 44 (43%) patients had pterygium form <
3 months while 58 (57%) patients had pterygium form > 3 months. Mean age was 3
months ± 2.16. Where as in group B 48 (47%) patients had pterygium form < 3 months while 54 (53%) patients
had pterygium form > 3 months.
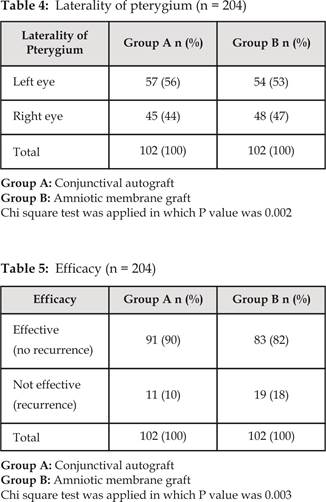
Mean age was 4 months ± 2.99 Table 3. Laterality of pterygium
among two groups was analyzed as in group
A 57 (56%) patients had pterygium in left eye and 45 (44%) patients had pterygium in right
eye. Where as in group B 54 (53%)
patients had pterygium in left eye and 48 (47%) patients had pterygium in right eye Table 4. Efficacy among
two groups was analyzed as conjunctival autograft was effective in 91 (90%) patients and was not
effective in 11 (10%) patients. Whereas amniotic membrane graft was effective in 83 (82%)
patients and was not effective in 19 (18%) patients Table 5.
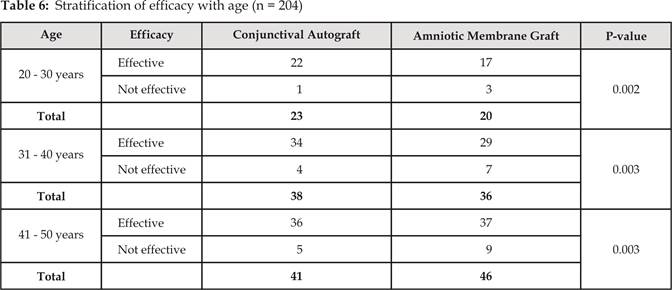
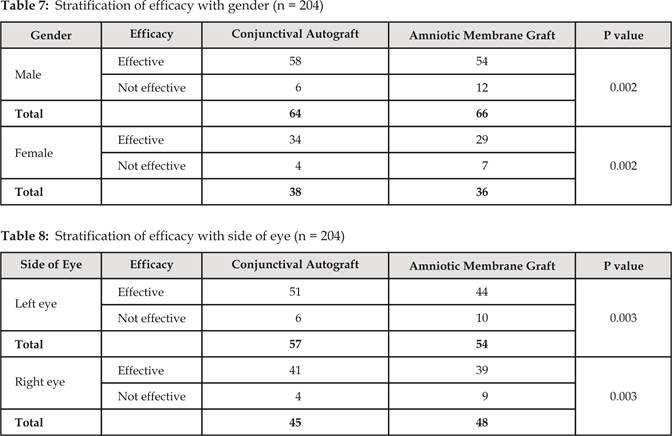
Stratification
of efficacy with age, gender and side
of the eye is given in Table 6-8.